Forteza et al from the Hospital Universitario 12 de Octubre described in this issue of the Revista Española de Cardiología their initial experience with aortic valve sparing operations for aortic root aneurysm in 18 patients with Marfan syndrome.1 The authors indicated that they have done 40 such operations for aortic root aneurysm. The early results reported are excellent and I commend them for introducing this type of conservative valve surgery in their cardiac unit. I have no doubt that in selected patients valve repair provides better clinical outcomes than valve replacement.
Aortic valve sparing operations are complicated procedures because they require exceptional knowledge of the functional anatomy of the aortic valve as well as technical expertise. They are not easily reproducible.
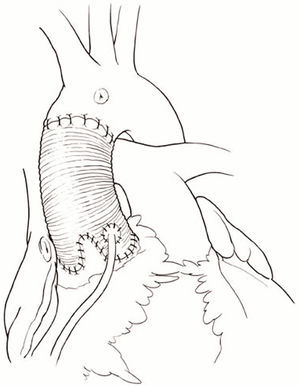
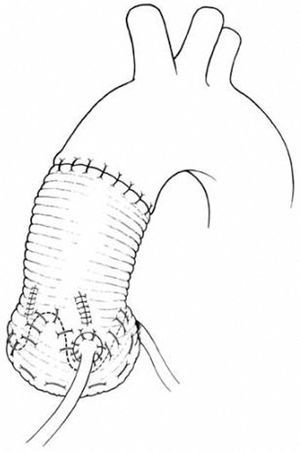
There are basically two types of aortic valve sparing operations to treat aortic root aneurysm: reimplantation of the aortic valve and remodeling of the aortic root.2 Figures 1, 2, and 3 show sketches of these operations. Remodeling of the aortic root is a physiologically sounder procedure than reimplantion of the aortic valve3 but we have shown in patients with Marfan syndrome that the aorto-ventricular junction continues to dilate after remodeling of the aortic root and eventually aortic insufficiency ensues.4 For this reason, we believe that reimplantation of the aortic valve is more appropriate to treat young patients with aortic root aneurysm whether they have the Marfan syndrome or not.5

Figure 1. Aortic root aneurysm and excision of the aneurysmal sinuses.

Figure 2. Remodeling of the aortic root.

Figure 3. Reimplantation of the aortic valve with creation of neo-aortic sinuses
Since the introduction of reimplantation of the aortic valve to treat aortic root aneurysms, several technical modifications have been proposed.6-8 Most of these changes have focused on creating neo-aortic sinuses to reduce the velocity of closure of the aortic cusps to hopefully enhance the durability of the procedure.9 Although we do not dispute that creating neo-aortic sinuses reduces the velocity of opening and closure of the aortic cusps, there is no evidence they enhance valve durability.5 Moreover, most surgeons, like the group from Hospital Universitario 12 de Octubre,1 use commercially available grafts with sinuses of Valsalva, which alter the anatomy of the aorto-ventricular junction. The aortic annulus is a tri-dimensional structure composed of 3 separate crescent shape structures that develop along a single plane, ie, each aortic cusp is inserted on a crescent shape structure on a single flat plane. The Valsalva graft changes that plane to a spherical one. Moreover, the height of each commissure is variable and that graft does not allow the surgeon to tailor the commissure correctly. Thus, we continue to use a straight tube to reimplant the aortic valve and create neo-aortic sinuses by plicating the spaces in between commissures as illustrated in Figure 1. This approach restores normal anatomy to the aorto-ventricular junction.
From 1988 to December 2006 we had performed 243 aortic valve-sparing operations for aortic root aneurysms and 40% of the patients had the stigmata of Marfan syndrome. The subgroup of patients with Marfan syndrome had a mean age of 35 (9) years and 10 patients were operated on as an emergency because of acute type A aortic dissection. The technique of remodeling of the aortic root was used in 22 patients and reimplantation of the aortic valve in 77. There was 1 operative death due a new acute type B aortic dissection. Patients have been followed from 1 to 216 months, mean of 69 months. There were only two late deaths, one due to rupture of the false lumen and the other due to chronic obstructive lung disease. The survival at 10 years was 95% (2). Four patients have required reoperation on the aortic valve, 3 for aortic insufficiency and 1 infective endocardits with aortic root abscess. All patients survived reoperation. In addition, one patient required mitral valve repair 8 years after aortic valve sparing operation for new mitral regurgitation and 3 patients required replacement of the entire thoracic aorta. No patient died but 1 became paraplegic. Annual echocardiographic studies have shown stable repair in all patients who had reimplantation of the aortic valve with only1 patient with moderate aortic insufficiency but normal left ventricular function and size. Eight patients out of 22 who had remodeling of the aortic root developed moderate or severe aortic insufficiency due to dilation of the aortic annulus 5 to 14 years after surgery.
Our experience supports the continued use of re-implantation of the aortic valve to treat aortic root aneurysm in patients with or without Marfan syndrome as long as the aortic cusps are normal or minimally stretched. Since dilation of the aortic annulus and/or sinotubular junction increases the mechanical stress on the aortic cusps, we believe that young patients with aortic root aneurysm should have surgery when the diameter of the aortic root reaches 50 mm.
See article on pages 471-5
Correspondence: Dr. Tirone E. David.
University of Toronto, 200 Elizabeth St. 4N457,
Toronto, Ontario, M5G 2C4, Canada.
E-mail: tirone.david@uhn.on.ca