
To analyze whether variations in physical activity (PA) and sedentary behaviors are accompanied by differences in maximal oxygen consumption (VO2max).
MethodsWe conducted a prospective cross-sectional study of 243 participants (82 women), aged 65.0±4.9 years old, with metabolic syndrome and overweight/obesity who performed a maximal exercise test with expired gas analysis. PA was evaluated using subjective methods, the REGICOR and RAPA 1 self-reported questionnaires, and objective methods, the chair test and accelerometry. Sedentariness was analyzed with the Nurses’ Health Study questionnaire and accelerometry.
ResultsVO2max was higher in participants who reported they adhered to the recommendations of the PA guidelines in the REGICOR questionnaire (21.3±4.6 vs 18.0±4.4 mL/kg/min; P <.001) and was 18% higher in those who reported more PA in the RAPA 1 questionnaire than the less active group (P <.001). The chair test (> 15 vs ≤ 15 repetitions) also showed significant differences in VO2max (21.2±4.8 vs 18.7±4.5 ml/kg/min; P <.001). Correlations between PA variables and VO2max were significant but low (r: 0.2 to 0.4). Sedentary activities showed less relationship with VO2max.
ConclusionsParticipants with metabolic syndrome and overweight/obesity who reported adhering to PA recommendations achieved higher VO2max. The self-reported questionnaires and the chair test identified significant variations in VO2max. Sedentary activities do not appear to modify VO2max.
Keywords
Physical fitness (PF) or cardiorespiratory functional capacity and physical activity (PA) are inversely and independently related to overall and cardiovascular mortality.1,2 However, PF seems to be a more powerful predictor of mortality,3,4 possibly because it can be more objectively determined than PA. In addition, sedentary behavior is a risk factor for cardiovascular disease and overall mortality.5,6 The promotion of PA is a universal recommendation for the prevention of cardiovascular diseases.7
The most objective method for measuring PF is the determination of maximal oxygen consumption (VO2max) through expired gas analysis. However, due to the complexity of its measurement, VO2max is rarely used in epidemiological studies. Accordingly, PA and sedentary behavior are typically evaluated with self-report questionnaires and objective methods such as pedometers or accelerometers. Although PA is the fundamental determinant of PF,8 the few studies to analyze their interrelationship have obtained discordant results,9,10 with the same inconsistency for the relationship between sedentary lifestyle and PF.9,11
From this perspective, we considered that it would be interesting to analyze the association of VO2max directly measured with cardiopulmonary exercise testing with PA and sedentary behavior in a population with high cardiovascular risk, namely, overweight or obese patients with metabolic syndrome (MetS), adhering to an exercise program. The results would allow us to determine whether PA could be used as an indirect measure of physical capacity. Therefore, the objective of this study was to verify whether changes in PA and sedentary behavior detected via questionnaires or accelerometry are accompanied by changes in VO2max.
METHODSStudy Design and ParticipantsThis prospective cross-sectional study was based on the data obtained from the participants of the Predimed-Plus trial at group allocation. This trial consists of a multicentre, randomized, parallel-group study of primary cardiovascular prevention that compares the effect on cardiovascular morbidity and mortality of an intensive lifestyle intervention based on a hypocaloric Mediterranean diet, increased PA, and behavioral therapy (intervention group) vs a nonintensive Mediterranean diet intervention without calorie restriction (control group). The participants comprised male volunteers aged 55 to 75 years or female volunteers aged 60 to 75 years with an overweight or obese status (body mass index [BMI] ≥ 27 and < 40) and at least 3 of the 5 components of MetS12 but without evidence of cardiovascular disease. The study has been described in greater detail elsewhere.13 The study was approved by the ethics committees of all participating centers and all volunteers signed a written consent form to confirm their voluntary participation. The study is registered in the International Standard Randomized Controlled Trials registry with the number 89898870.
Exercise Test With Gas AnalysisA symptom-limited maximal treadmill test was performed (General Electric model T2100) according to the Bruce ramp protocol and with continuous electrocardiographic monitoring. The participants were asked to exert themselves until they were exhausted; they were allowed to support themselves on the handrails without holding on. Blood pressure and heart rate were recorded every 3minutes and at the end of the test. Expired gas analysis was performed using a system for metabolic tests (MetaSoft CPX testing, GE Medical Systems Information Technologies; Freiburg, Germany) with a gas analyzer (MetaLyzer 3B, Firmware Version 2.0, CORTEX; Leipzig, Germany).
Effort was considered maximal when the respiratory exchange ratio exceeded 1.10.14 When the respiratory exchange ratio was between 1 and 1.10, effort was only considered adequate for inclusion in the present analysis if the heart rate was ≥ 90% of the theoretical maximum (220 bpm – age) and the Borg scale score was ≥ 17.14,15 The value obtained at the final moment of the exercise was considered to be the VO2max for that individual. Based on the Wasserman equations,16 the device software calculated the workload, expressed as metabolic equivalents (1 MET = 3.5mL O2/kg/min) and the predicted VO2max.
Physical Activity and Sedentary Behavior QuestionnairesSelf-reported PA was evaluated using the REGICOR17 and RAPA18 questionnaires.
The REGICOR questionnaire, recently validated in Spain, is based on a population study and includes the version validated for Spain of the Minnesota Leisure-time Physical Activity Questionnaire. It collects information on the type of leisure-time PA, its frequency (d/wk), and its duration (min/d). Intensity was evaluated according to the 2011 Compendium of Physical Activities.19 According to intensity, activities were classified as light (< 4 MET), moderate (4-5.5 MET), and vigorous (> 6 MET).20 These data allowed PA to be dichotomized according to the clinical practice guideline recommendations for leisure-time PA4,7: moderate-vigorous PA ≥ 150min/wk or vigorous PA ≥ 75min/wk or energy expenditure ≥ 500 MET min/wk.
The RAPA questionnaire consists of 7 questions related to aerobic or dynamic PA (RAPA 1) and 2 questions on activities that increase muscle strength and improve balance (RAPA 2). The RAPA 1 also establishes 3 levels of PF (1, 2, and 3) from lowest to highest. Level 3 questions consider the clinical practice guideline recommendations.
Sedentary behavior was evaluated through the Nurses’ Health Study questionnaire validated for Spain21; of the sedentary activities considered, the time spent sitting in hours per day (≥ 7h) and the television viewing time grouped into 3 categories were selected: ≤ 2, 2 to 4, and > 4h/d.20
Objective MethodsThe Predimed-Plus trial included the “chair test”. This PF test evaluates lower body strength by recording the number of times participants can sit down and get up from a standard-size chair (43-44cm in height) for 30seconds. The reference values for the Spanish population have been published.22 According to the number of repetitions and patients’ age and sex, PF was classified into 3 levels (1, 2, and 3) from lowest to highest. For the present analysis, 15 was selected as the cutoff point to consider an individual to be in good PF, taking into account the mean age of the study population. According to the results of the chair test and RAPA 1, in the Predimed-Plus trial, a final classification was established in 3 levels: lightly active, moderately active, and active.
The study protocol also included accelerometry in a subsample of the participants (20% of the control group and 50% of the intervention group). The GENEActiv GATV04 accelerometer (Activinsights Ltd; Kimbolton, United Kingdom) was used over a 7-day monitoring period. The data were processed in R (R Core Team; Vienna, Austria) using the GGIR package (version 1.2-5). The cutoff points for moderate/vigorous PA were as published.23
Statistical AnalysisCategorical variables are reported as frequencies and percentages and continuous variables as mean ± standard deviation. Comparisons between groups were made by the t test or ANOVA (analysis of variance) for continuous data and by the chi-square test for categorical data.
The Pearson correlation coefficient was used to assess the association between the PF variables obtained in cardiopulmonary exercise testing (VO2max and MET) and the continuous variables of PA and sedentary lifestyle. For variables that were by definition categorical (RAPA and RAPA+Chair), the association was determined by the eta correlation coefficient.
The possible influence of PA and sedentary lifestyle variables on VO2max was analyzed according to a 3-step process: first, univariable linear regressions were performed that included the dependent variable VO2max and each variable of PA that had shown a significant correlation as an independent variable; second, linear multivariable models were performed that included, apart from the independent variable, age and sex as potentially confounding variables; and finally, a multivariable model was applied that included, in addition to the variables included in the previous step, BMI as a possible confounding variable. In the models using the RAPA scale as an independent variable, “lightly active” was considered the reference category.
All statistical analyses were performed with SPSS 23 software.
RESULTSFrom September 2014 to November 2016, 274 patients were selected; 243 of these patients underwent adequate cardiopulmonary exercise testing for their analysis in the present study. The following patients were excluded: 3 who did not undergo the exercise test, 2 who could not tolerate the oxygen mask, and 24 did not exert enough effort according to the previously established criteria; in addition, there were technical problems in 2 tests.
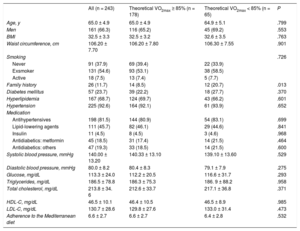
The participants’ baseline characteristics are shown in Table 1. The mean age was 65 ± 4.9 years, 66% of the participants were men, and the mean BMI indicated obesity (32.5 ± 3.3). To provide more detailed information, participants were divided into 2 groups according to whether their functional aerobic capacity was preserved or decreased (≥ 85% or < 85% of the predicted VO2max).24 There were no significant differences between the groups in the anthropometric variables, classic cardiovascular risk factors—except family history of early ischemic heart disease——, pharmacological treatment, basal glycemia, or lipid profile.
Participants’ Baseline Characteristics
| All (n = 243) | Theoretical VO2max ≥ 85% (n = 178) | Theoretical VO2max < 85% (n = 65) | P | |
|---|---|---|---|---|
| Age, y | 65.0 ± 4.9 | 65.0 ± 4.9 | 64.9 ± 5.1 | .799 |
| Men | 161 (66.3) | 116 (65.2) | 45 (69.2) | .553 |
| BMI | 32.5 ± 3.3 | 32.5 ± 3.2 | 32.6 ± 3.5 | .763 |
| Waist circumference, cm | 106.20 ± 7.70 | 106.20 ± 7.80 | 106.30 ± 7.55 | .901 |
| Smoking | .726 | |||
| Never | 91 (37.9) | 69 (39.4) | 22 (33.9) | |
| Exsmoker | 131 (54.6) | 93 (53.1) | 38 (58.5) | |
| Active | 18 (7.5) | 13 (7.4) | 5 (7.7) | |
| Family history | 26 (11.7) | 14 (8.5) | 12 (20.7) | .013 |
| Diabetes mellitus | 57 (23.7) | 39 (22.2) | 18 (27.7) | .370 |
| Hyperlipidemia | 167 (68.7) | 124 (69.7) | 43 (66.2) | .601 |
| Hypertension | 225 (92.6) | 164 (92.1) | 61 (93.9) | .652 |
| Medication | ||||
| Antihypertensives | 198 (81.5) | 144 (80.9) | 54 (83.1) | .699 |
| Lipid-lowering agents | 111 (45.7) | 82 (46.1) | 29 (44.6) | .841 |
| Insulin | 11 (4.5) | 8 (4.5) | 3 (4.6) | .968 |
| Antidiabetics: metformin | 45 (18.5) | 31 (17.4) | 14 (21.5) | .464 |
| Antidiabetics: others | 47 (19.3) | 33 (18.5) | 14 (21.5) | .600 |
| Systolic blood pressure, mmHg | 140.00 ± 13.20 | 140.33 ± 13.10 | 139.10 ± 13.60 | .529 |
| Diastolic blood pressure, mmHg | 80.0 ± 8.2 | 80.4 ± 8.3 | 79.1 ± 7.9 | .275 |
| Glucose, mg/dL | 113.3 ± 24.0 | 112.2 ± 20.5 | 116.6 ± 31.7 | .293 |
| Triglycerides, mg/dL | 186.5 ± 78.8 | 186.3 ± 75.3 | 186. 9 ± 88.2 | .958 |
| Total cholesterol, mg/dL | 213.8 ± 34. 6 | 212.6 ± 33.7 | 217.1 ± 36.8 | .371 |
| HDL-C, mg/dL | 46.5 ± 10.1 | 46.4 ± 10.5 | 46.5 ± 8.9 | .985 |
| LDL-C, mg/dL | 130.7 ± 28.6 | 129.8 ± 27.6 | 133.0 ± 31.4 | .473 |
| Adherence to the Mediterranean diet | 6.6 ± 2.7 | 6.6 ± 2.7 | 6.4 ± 2.8 | .532 |
BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein-cholesterol; VO2max, maximal oxygen consumption.
Continuous values are presented as mean ± standard deviation and categorical as No. (%).
Table 2 shows the variations in the PF evaluated by the VO2max and METs achieved in the exercise test with the PA, sedentary behavior, and the chair test variables, categorized as explained in the “Methods”, with special reference to guideline recommendation adherence. Individuals who reported adhering to the clinical practice guideline recommendations in the REGICOR questionnaire (moderate-vigorous PA ≥ 150min/wk or vigorous PA ≥ 75min/wk) had higher aerobic capacity (P < .001) with a difference in VO2max of 3.1 to 3.2mL O2/kg/min, which represents a difference of 17% to 18% in the VO2max reached vs those not adhering to the recommendations. The RAPA questionnaire showed similar differences between the active group (meeting guidelines) and the lightly active group (differences of 3.3mL O2/kg/min and 18%). However, participants’ self-reported sedentary behavior did not seem to be related to functional capacity.
Association Between Physical Fitness Variables (VO2max and MET) and Physical Activity, Sedentary Lifestyle, and Chair Test Variables
| No. | VO2max | P | MET | P | |
|---|---|---|---|---|---|
| Questionnaire variables completed by participants | |||||
| *Moderate-vigorous PA | < .001 | < .001 | |||
| < 150 min/wk | 127 | 18.0 ± 4.4 | 9.1 ± 2.1 | ||
| ≥ 150 min/wk | 116 | 21.3 ± 4.6 | 10.9 ± 2.4 | ||
| *Vigorous PA | < .001 | < .001 | |||
| < 75 min/wk | 167 | 18.5 ± 4.3 | 9.5 ± 2.3 | ||
| ≥ 75 min/wk | 76 | 21.7 ± 5.0 | 11.2 ± 2.2 | ||
| PA time | < .001 | .001 | |||
| < 60 min/d | 159 | 18.4 ± 4.3 | 9.6 ± 2.2 | ||
| ≥ 60 min/d | 84 | 21.8 ± 4.8 | 10.7 ± 2.6 | ||
| Total energy expenditure | < .001 | .002 | |||
| < 500 MET min/wk | 42 | 18.2 ± 4.5 | 8.9 ± 2.0 | ||
| ≥ 500 MET min/wk | 201 | 20.8 ± 4.7 | 10.2 ± 2.4 | ||
| *Moderate-vigorous energy expenditure | < .001 | < .001 | |||
| < 500 MET min/wk | 100 | 17.8 ± 4.3 | 9.0 ± 2.2 | ||
| ≥ 500 MET min/wk | 143 | 19.7 ± 4.8 | 10.1 ± 2.5 | ||
| RAPA | < .001 | < .001 | |||
| Level 1 (lightly active) | 96 | 17.9 ± 4.2 | 8.9 ± 2.0 | ||
| Level 2 (moderately active) | 59 | 19.7 ± 4.6 | 10.2 ± 2.0 | ||
| Level 3 (active) | 88 | 21.2 ± 4.9 | 11.2 ± 2.5 | ||
| *Dichotomous RAPA 1 | < .001 | < .001 | |||
| Lightly active-moderately active | 155 | 18.6 ± 4.4 | 9.4 ± 2.1 | ||
| Active | 88 | 21.2 ± 4.9 | 11.0 ± 2.5 | ||
| Sitting position | .055 | .182 | |||
| < 7 h/d | 114 | 20.2 ± 4.6 | 10.2 ± 2.4 | ||
| ≥ 7 h/d | 129 | 19.0 ± 4.8 | 9.8 ± 2.3 | ||
| Sedentary behavior, h TV/d | .310 | .064 | |||
| ≤ 2 h TV/d | 5 | 22.5 ± 4.5 | 9.1 ± 2.3 | ||
| 2-4 h TV/d | 41 | 19.9 ± 5.0 | 10.7 ± 2.4 | ||
| ≥ 4 h TV/d | 197 | 19.4 ± 4.7 | 9.9 ± 2.4 | ||
| Variables obtained by objective methods | |||||
| Chair test | < .001 | < .001 | |||
| ≤ 15 | 156 | 18.6 ± 4.5 | 9.4 ± 2.1 | ||
| > 15 | 87 | 21.2 ± 4.8 | 11.1 ± 2.4 | ||
| Chair test+RAPA | < .001 | < .001 | |||
| Lightly active | 106 | 18.1 ± 4.1 | 9.0 ± 2.0 | ||
| Moderately active | 68 | 20.1 ± 4.8 | 10.4 ± 2.2 | ||
| Active | 69 | 21.2 ± 4.9 | 11.1 ± 2.5 | ||
| Moderate-vigorous PA (accelerometry) | .283 | .312 | |||
| < 150 min/wk | 63 | 19.9 ± 4.7 | 10.1 ± 2.2 | ||
| ≥ 150 min/wk | 28 | 21.1 ± 4.7 | 10.6 ± 2.6 | ||
| Sedentary behavior (accelerometry) | .624 | .067 | |||
| < 420 min | 7 | 19.5 ± 5.4 | 10.3 ± 2.5 | ||
| ≥ 420 min | 84 | 20.4 ± 4.7 | 10.2 ± 2.3 | ||
MET, metabolic equivalent; PA, physical activity; TV, television; VO2max, maximal oxygen consumption.
The objective methods also detected significant differences (P < .001), both with the dichotomized chair test data (> 15 or ≤ 15 repetitions) and with the combined results of the chair test classification and the RAPA 1 questionnaire (differences of 3.1mL O2/kg/min and 17% between the active and lightly active groups). However, accelerometry failed to detect differences in VO2max with either moderate-vigorous PA or sedentary behavior.
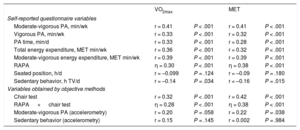
Table 3 shows the correlation between VO2max and METs with the PA, sedentary lifestyle, and chair test variables analyzed in Table 2. Moderate-vigorous PA declared in the REGICOR questionnaire showed the highest correlation coefficient (r = 0.41), whereas sedentary activity (hours watching television per day) reached –0.14, indicating borderline significance.
Correlation Coefficients Between Physical Fitness Variables (VO2max and MET) and Physical Activity, Sedentary Lifestyle, and Chair Test Variables
| VO2max | MET | |||
|---|---|---|---|---|
| Self-reported questionnaire variables | ||||
| Moderate-vigorous PA, min/wk | r = 0.41 | P < .001 | r = 0.41 | P < .001 |
| Vigorous PA, min/wk | r = 0.33 | P < .001 | r = 0.32 | P < .001 |
| PA time, min/d | r = 0.33 | P < .001 | r = 0.28 | P < .001 |
| Total energy expenditure, MET min/wk | r = 0.36 | P < .001 | r = 0.32 | P < .001 |
| Moderate-vigorous energy expenditure, MET min/wk | r = 0.39 | P < .001 | r = 0.39 | P < .001 |
| RAPA | η = 0.30 | P < .001 | η = 0.38 | P < .001 |
| Seated position, h/d | r = –0.099 | P = .124 | r = –0.09 | P = .180 |
| Sedentary behavior, h TV/d | r = –0.14 | P = .034 | r = –0.16 | P = .015 |
| Variables obtained by objective methods | ||||
| Chair test | r = 0.32 | P < .001 | r = 0.42 | P < .001 |
| RAPA + chair test | η = 0.28 | P < .001 | η = 0.38 | P < .001 |
| Moderate-vigorous PA (accelerometry) | r = 0.20 | P = .058 | r = 0.22 | P = .038 |
| Sedentary behavior (accelerometry) | r = 0.15 | P = .145 | r = 0.002 | P = .984 |
MET, metabolic equivalent; PA, physical activity; TV, television; VO2max, maximal oxygen consumption.
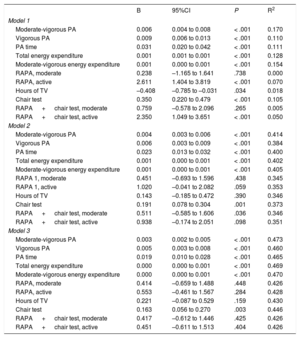
A multivariable analysis was performed using the variables showing a significant correlation with VO2max in the univariable analysis. After adjustment for age, sex, and BMI (Table 4), there was still a positive and statistically significant association with the PA recorded in the REGICOR questionnaire, for both intensity (moderate-vigorous PA, vigorous PA, moderate-vigorous energy expenditure) and time (PA time, total energy expenditure). The chair test was also statistically significant in the multivariable analysis. In contrast, the RAPA questionnaire, the combined RAPA questionnaire and chair test, and sedentary behavior evaluated by hours watching television were no longer significant.
Regression Analysis of VO2max With Physical Activity, Sedentary Lifestyle, and Chair Test Variables
| B | 95%CI | P | R2 | |
|---|---|---|---|---|
| Model 1 | ||||
| Moderate-vigorous PA | 0.006 | 0.004 to 0.008 | < .001 | 0.170 |
| Vigorous PA | 0.009 | 0.006 to 0.013 | < .001 | 0.110 |
| PA time | 0.031 | 0.020 to 0.042 | < .001 | 0.111 |
| Total energy expenditure | 0.001 | 0.001 to 0.001 | < .001 | 0.128 |
| Moderate-vigorous energy expenditure | 0.001 | 0.000 to 0.001 | < .001 | 0.154 |
| RAPA, moderate | 0.238 | –1.165 to 1.641 | .738 | 0.000 |
| RAPA, active | 2.611 | 1.404 to 3.819 | < .001 | 0.070 |
| Hours of TV | –0.408 | –0.785 to –0.031 | .034 | 0.018 |
| Chair test | 0.350 | 0.220 to 0.479 | < .001 | 0.105 |
| RAPA + chair test, moderate | 0.759 | –0.578 to 2.096 | .265 | 0.005 |
| RAPA + chair test, active | 2.350 | 1.049 to 3.651 | < .001 | 0.050 |
| Model 2 | ||||
| Moderate-vigorous PA | 0.004 | 0.003 to 0.006 | < .001 | 0.414 |
| Vigorous PA | 0.006 | 0.003 to 0.009 | < .001 | 0.384 |
| PA time | 0.023 | 0.013 to 0.032 | < .001 | 0.400 |
| Total energy expenditure | 0.001 | 0.000 to 0.001 | < .001 | 0.402 |
| Moderate-vigorous energy expenditure | 0.001 | 0.000 to 0.001 | < .001 | 0.405 |
| RAPA 1, moderate | 0.451 | –0.693 to 1.596 | .438 | 0.345 |
| RAPA 1, active | 1.020 | –0.041 to 2.082 | .059 | 0.353 |
| Hours of TV | 0.143 | –0.185 to 0.472 | .390 | 0.346 |
| Chair test | 0.191 | 0.078 to 0.304 | .001 | 0.373 |
| RAPA + chair test, moderate | 0.511 | –0.585 to 1.606 | .036 | 0.346 |
| RAPA + chair test, active | 0.938 | –0.174 to 2.051 | .098 | 0.351 |
| Model 3 | ||||
| Moderate-vigorous PA | 0.003 | 0.002 to 0.005 | < .001 | 0.473 |
| Vigorous PA | 0.005 | 0.003 to 0.008 | < .001 | 0.460 |
| PA time | 0.019 | 0.010 to 0.028 | < .001 | 0.465 |
| Total energy expenditure | 0.000 | 0.000 to 0.001 | < .001 | 0.469 |
| Moderate-vigorous energy expenditure | 0.000 | 0.000 to 0.001 | < .001 | 0.470 |
| RAPA, moderate | 0.414 | –0.659 to 1.488 | .448 | 0.426 |
| RAPA, active | 0.553 | –0.461 to 1.567 | .284 | 0.428 |
| Hours of TV | 0.221 | –0.087 to 0.529 | .159 | 0.430 |
| Chair test | 0.163 | 0.056 to 0.270 | .003 | 0.446 |
| RAPA + chair test, moderate | 0.417 | –0.612 to 1.446 | .425 | 0.426 |
| RAPA + chair test, active | 0.451 | –0.611 to 1.513 | .404 | 0.426 |
95%CI, 95% confidence interval; PA, physical activity; TV, television; VO2max, maximal oxygen consumption.
Model 1: without adjustment. Model 2: adjusted for age and sex. Model 3: adjusted for age, sex, and body mass index. RAPA: the “lightly active” category was used as reference.
In overweight or obese patients with MetS, PA assessed by the self-reported REGICOR and RAPA questionnaires allowed detection of significant differences in VO2max that were greater than 15% between those reporting more leisure-time PA and the less active, with similar results obtained with the chair test. Thus, PA generally has a significant, although not strong, relationship with PF. In contrast, sedentary behavior showed a weaker relationship with VO2max.
Regarding the MethodsAlthough VO2max is the parameter of choice for evaluating PF or cardiorespiratory functional capacity, its determination is difficult because it requires specialized technology and personnel. An alternative method is to use the duration of the exercise test without expired gas analysis or the METs reached at peak effort estimated from the speed and slope of the treadmill or bicycle watts; the high correlation coefficients of the 2 variables with VO2max justify their use.25 Indeed, METs are the most widely used indicator of PF in the literature.26 For this reason, METs were included in this analysis and their results were comparable to those of VO2max (Table 2 and Table 3), although they overestimate PF vs measured VO2max, as can also be seen from the results obtained. The entire group achieved 10 ± 2.4 METs with a VO2max of 19.6 ± 4.7mL/kg/min, representing an overestimation of 45%.
Physical Activity and Physical Form (VO2max)The REGICOR and RAPA questionnaires provided adequate information on PF and, in particular, on the VO2max and METs reached at maximal effort. Individuals who reported that they adhered to the clinical practice guideline recommendations regarding leisure-time PA had a VO2max 17% to 18% higher than those who did not, representing a difference of 3.1 to 3.2mL/kg/min in absolute numbers, with the same result for comparison of the most and least active groups when the variable had 3 categories. These results are clinically relevant because a 1 MET (3.5mL O2/kg/min) increment in PF is accompanied by 10% to 25% reductions in mortality.1,5 Additionally, in this study, the time spent on leisure-time PA, regardless of its intensity, was significantly related to VO2max, both in the univariable analysis and after adjustment for age, sex, and BMI, with the same findings for total energy expenditure. These results indicate that light PA, not just moderate and/or vigorous activity, may have beneficial effects, as indicated by recent work.27
Analysis of the correlation between the PA recorded in the questionnaires and VO2max revealed that the results agree with those in the literature. The correlation coefficients range between 0, 1, and 0.4 for both measured9,27 and estimated VO2max,3,10 with vigorous PA at the upper end of these values.28 Objective methods do not substantially improve upon the results obtained with the questionnaires. For example, in a study of 1631 young Australians, Schmidt et al.29 obtained correlation coefficients of 0.16 for men and 0.19 for women using pedometers, whereas Dyrstad et al.9 determined correlation coefficients of 0.47 for men and 0.54 for women using accelerometers. Our accelerometry results (r = 0.22) may have been influenced by the small number of patients tested, although the specific results for the 91 individuals who wore the accelerometers are in line with the positive results of the questionnaires in Table 2 (). No explanation was found for the apparent superiority of the questionnaires over accelerometry in the present study, which has robustly compared the usefulness of both methods.
In contrast, the chair test, an easy-to-implement functional test that assesses lower body strength, together with the moderate-vigorous PA of the questionnaires, was the parameter showing the best correlation with VO2max in the univariable analysis and remained significant in the regression analysis. The step test, another method that assesses the lower body, has also shown a positive association with PF.30
Leaving aside the possible influence of the various methods and tests used, these results seem to indicate that the 2 variables being evaluated, although related, are nonetheless markedly different. PA is a multidimensional behavior defined as any movement that increases basal energy expenditure, whereas VO2max is a physiological parameter that reflects the ability of the cardiorespiratory and circulatory system to transport oxygen to cells. The latter has an important genetic component31 that determines individual response to physical exercise.
Sedentary Behavior and Physical Fitness (VO2max)A surprising finding was the slight or absent relationship between sedentary behavior and VO2max. The only parameter inversely related to PF was the number of hours watching television, but this correlation was slight (r = –0.14) and lost statistical significance in the regression analysis. The number of hours sitting per day was not related to VO2max, as assessed by both questionnaire and accelerometry. Similar results have been published in a study9 that measured the sedentary behavior of 759 Norwegian adults with accelerometers, with no significant differences in hours of sedentary behavior between participants with higher and lower VO2max values. Perhaps the type of sedentary behavior should be taken into account. Indeed, Saidj et al.6 found that the time spent sitting at work was not related to VO2max, whereas leisure-time sedentary behavior had an inverse and significant relationship.
Study LimitationsThe interpretation of these results was complicated by the small number of participants in some subgroups. In addition, although a significant number of participants had MetS and were overweight, this is a specific population group and the application of the conclusions to other groups would be inappropriate. The present analysis was performed by a single research group, which is usually an inconvenience when it comes to the generalization of results but is a positive aspect in this case because of the reduced variability in the performance of exercise tests with expired gas analysis. Finally, this study was cross-sectional and the level of evidence of the results would have been higher with a longitudinal design.
CONCLUSIONSThe PA, REGICOR, and RAPA self-reported questionnaires, as well as the chair test, reflect significant variations in PF (VO2max and MET) between overweight or obese individuals with MetS who report higher PA and those who are less active and between those who reported adhering to PA recommendations and those who do not. These findings are interesting because the direct VO2max determination is complex and cannot be applied to large population groups. However, the association between PA and PF is not strong enough for these variables to replace one another, although the questionnaires and the chair test can be useful for monitoring patients in training and rehabilitation programs. A sedentary lifestyle had little relationship with PF.
FUNDINGThe present work was funded by the Instituto de Salud Carlos III (ISCIII) (Spanish Ministry of Economy, Industry, and Competitiveness) through an FIS (Fondo de Investigación Sanitaria) project coordinated by J. Salas-Salvadó (PI13/01056) and by the Centro de Investigación Biomédica en Red de la Fisiopatología de la Obesidad y Nutrición (CIBEROBN).
CONFLICTS OF INTERESTJ. Salas-Salvadó has received grants from the ISCIII (Spanish Ministry of Economy, Industry, and Competitiveness)—RTIC G03/140 ISCIII and CIBEROBN—during the study period. Apart from the present study, he declares noneconomic support from the Nut and Dried Fruit Foundation; fees from Danone Institute, Danone SA, Font Vella Lanjarón, Nuts for Life, Eroski Distributors; and grants from the Nut and Dried Fruit Foundation and Eroski Distributors.
F. Arós has received grants from the ISCIII (Spanish Ministry of Economy, Industry, and Competitiveness)—FIS (PI13/01056) and CIBEROBN—during the study period.
- –
PF or physical capacity and PA are inversely and independently associated with overall and cardiovascular mortality, although PF is a more powerful predictor. A sedentary lifestyle is also associated with worse prognosis.
- –
Encouragement of PA and the fight against sedentary behavior are public health policies endorsed by scientific societies.
- –
No universally accepted procedures allow the accurate and reliable evaluation of these variables.
- –
The self-reported PA, REGICOR, and RAPA questionnaires are short and easy to apply and detect significant variations in PF evaluated with VO2max and MET in overweight or obese patients with MetS. The same occurs with the chair test.
- –
The individuals of this group who reported adherence to clinical practice guideline recommendations regarding leisure-time PA showed significantly higher PF than those not adhering to the guidelines.
- –
The correlation between PF and PA does not allow the indiscriminate use of the 2 variables in overweight or obese patients with MetS.