

Adults with disability have higher risk of all-cause mortality, but evidence on their risk of cardiovascular mortality is scarce. This study aimed to evaluate the association between disability severity and mortality from cardiovascular causes among community-dwelling adults.
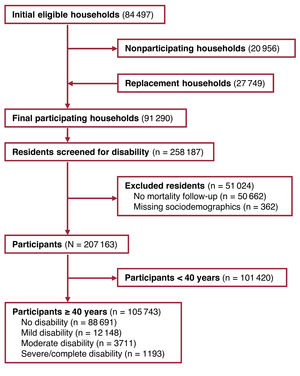
MethodsA representative cohort of 105 743 community-dwelling Spanish adults aged 40 years or older was screened for disability severity within the framework of the international classification of functioning, disability, and health from 2007 to 2008 and was followed up for cardiovascular mortality until 2017. Five- and 10-year cardiovascular mortality risks in each disability category were standardized by sociodemographic characteristics using inverse probability weighting and corrected for competing causes of death. Bias analyses were performed to quantify residual confounding by unmeasured baseline cardiovascular conditions.
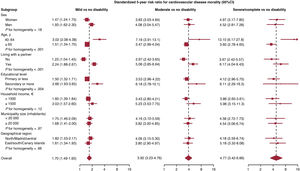
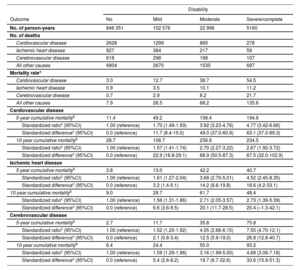
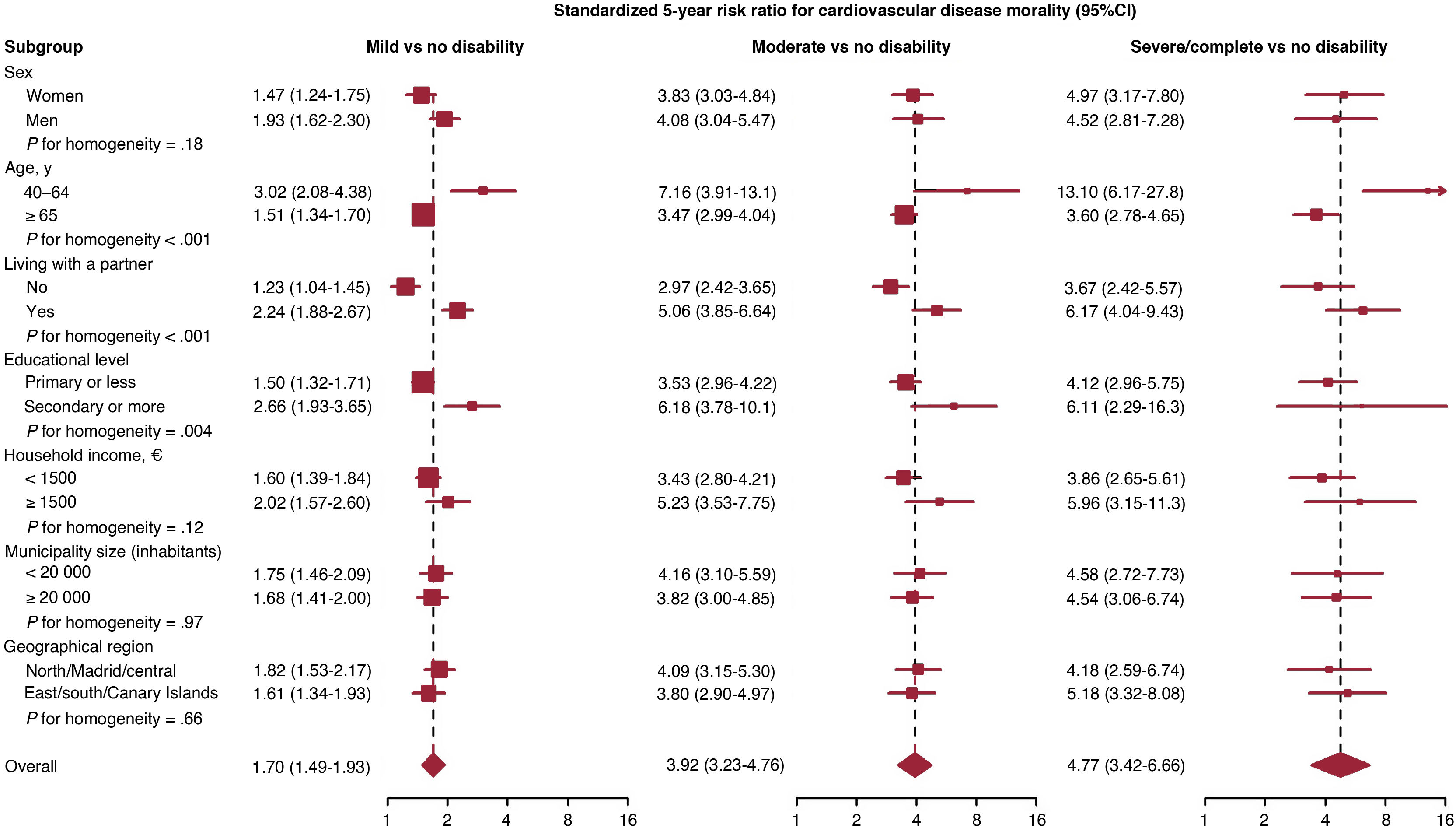
ResultsThe baseline prevalence of disability was 16.2% (95%CI, 15.9-16.4), including 11.5% with mild, 3.5% with moderate, and 1.1% with severe/complete disability. Compared with no disability, the standardized 5-year risk ratios for cardiovascular mortality (95%CI) were 1.70 (1.49-1.93), 3.92 (3.23-4.76), and 4.77 (3.42-6.66) for mild, moderate, and severe/complete disability, respectively, corresponding to 11.7 (8.4-15.0), 49.0 (37.0-60.9), and 63.1 (37.0-89.3) excess cardiovascular deaths per 1000 persons. The positive confounding in these risk ratios by unmeasured prevalent cardiovascular conditions was 5.9%. Results were similar for ischemic heart disease and cerebrovascular mortality and were sustained after 10 years of follow-up.
ConclusionsAdults with disability have higher mortality from cardiovascular causes. Conditions that increase cardiovascular risk in people with disability should be investigated. Preventive measures and health promotion initiatives are needed to reduce the risk of cardiovascular mortality in this population.
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm