Cardiovascular disease (CVD) is the leading cause of death in high-income countries such as Spain, as well as low- and middle-income countries.1 In Spain, CVD has continued to rank as the number one cause of death for the last several decades. Large differences between countries in terms of CVD mortality have been described.2 Spain, along with France, Japan, and Italy, are considered low-risk CVD countries.3 Two disease categories account for the vast majority of cardiovascular disease events: namely coronary heart disease (CHD) and stroke.
In this issue of Revista Española de Cardiología, Flores-Mateo et al.4 shed new light on the factors underlying the reduction of CHD mortality in a low-risk country such as Spain during the period of 1988-2005. By using the IMPACT model5 they have quantified the contribution of relevant CHD risk factors and evidence-based therapies to the overall decline of CHD mortality. This model has been applied and validated in other countries, such as the United States, Finland, the United Kingdom, and Italy. The IMPACT model aggregates risk factors (total cholesterol, systolic blood pressure, smoking, diabetes, body mass index, and physical inactivity) and evidence-based therapies (management of acute coronary syndromes, secondary prevention therapies, chronic angina, and heart failure treatments and the control of hypertension and hyperlipidemia) to disentangle the contribution of each factor to the variation in CHD mortality.
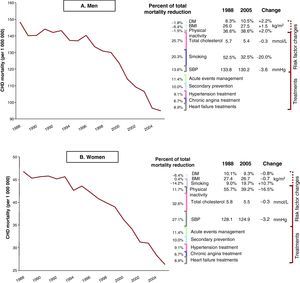
According to the study by Flores-Mateo et al.,4 52% of the decline in CHD mortality can be explained by population-wide risk factor changes over time whereas CHD evidence-based therapies for patients with established disease have contributed the remaining 48% (Figure 1). The largest contributor to the mortality decline in Spain was the improvement in total cholesterol levels that is estimated to have prevented or postponed 23.9% of deaths, while improvements in systolic blood pressure may have accounted for 14.9% of CHD mortality decline. These results also highlight the fact that not all risk factors have followed the beneficial trends for CHD. The increases observed in body mass index in men, smoking in women, and diabetes in both sexes have hindered the CHD mortality decline in Spain. Among evidence-based therapies, the management of acute coronary syndromes (acute myocardial infarction and unstable angina) prevented or postponed 11% of CHD deaths whereas secondary prevention (after infarction or revascularization) was responsible for 10% of such decline.

Figure 1. Coronary heart disease mortality decline in Spanish men (A) and women (B) from 1988 to 2005 as explained by risk factor changes and evidence-based therapies. DM, diabetes mellitus; BMI, body mass index; CHD, coronary heart disease; SBP, systolic blood pressure.
The results of the Flores-Mateo et al. study4 are consistent with the application of the IMPACT model in other populations and with a recently published analysis of a British cohort attributing 48% of the decline in CHD mortality to changes in CHD risk factors.6
Both population-wide improvements in CHD risk factors and improved delivery of evidence-based therapies (by increasing the percentage of patients receiving them and by improving adherence) are key points to progress in CHD prevention.7
Several relevant points for the prevention of CHD in Spain are raised in this elegant application of the IMPACT methodology:
• CHD risk factors such as body weight, diabetes mellitus, and smoking continue to impede the decline of CHD mortality in Spain.
• Relevant sex differences in terms of risk factor distribution should be acknowledged.
• There is great room for improvement of CHD evidence-based therapies uptake and adherence.
• Health policies directly related with cardiovascular prevention may offer great opportunities in Spain.
• Spain, along with other high-income countries, is in need of a state-of-the-art CVD surveillance network.
As Flores-Mateo et al.4 report, increasing body weight, diabetes, and smoking contributed to rising CHD deaths in Spain. (Doted lines in Figure 1) This phenomenon has been previously well described in the United States.8 Special strategies should be implemented to tackle smoking, diabetes, and obesity, which represent our main opportunity for CHD prevention in the coming decades.
It is interesting to note the sex differences in the distribution of CHD risk factors (Panels A and B in Figure 1). Smoking rates have steadily decreased in men (from 52.5% in 1988 to 32.5% in 2005) while they have increased in women (from 9% in 1988 to 19.7% in 2005) during the last decades in Spain. In a similar British study,6 smoking trends decreased in both sexes. Prevention programs should acknowledge relevant sex differences. There are also important sex differences regarding evidence-based therapies. The current analysis does not address possible differences between sexes in therapy uptake, which may be relevant, especially when it comes to the management of acute coronary syndromes.9
Evidence-based therapies are also a cornerstone of CHD mortality prevention,10 as this study and the previous IMPACT applications have consistently shown.7
The design and evaluation of programs aimed at improving therapies uptake and adherence should be one of our main foci. Previous attempts have shown increasing success in the control of CHD risk factors such as hypertension by using multifactorial interventions to increase adherence to treatment within the primary care system.11
Previous health policy driven population-wide interventions have proven effective at reducing CHD mortality.12 Public health has always been a hybrid discipline, using the tools of biological science and statistics to build the required knowledge base and then applying this knowledge in the world of politics and social relations. The knowledge required for cardiovascular disease prevention is now available; however, policy interventions have fallen short. Prevention of CHD in Spain will require a set of health policies to ensure the adoption of healthy lifestyles. The basic elements of such policies are outlined in Table 1, differentiating 3 levels of action – the policymaking, health systems, and individual levels, helping individuals to sustain the necessary behavior changes.10 A contemporary example of a public health intervention directed to children that integrates all aspects of individual behavior changes in Spain is the SI! (Salud Integral) program, sponsored by the SHE foundation,13 which undertakes the task of promoting cardiovascular health among school children.
Table 1. Public Health Interventions by Specific Cardiovascular Disease Risk Factors at Three Levels: Policy, Health System, and Behavioral Change.
| CVD risk factors | Policy level interventions | Health systems strengthening and integration | Behavior change interventions |
| Smoking | Tobacco controlPrograms for children and adolescents | Primary care programs for smoking cessation | Avoiding smoking uptake by young individualsSmoking cessation |
| Physical inactivity | Built environment policiesRecreational facilitiesPromoting walking and bicycling as means of transportation | Primary care programs for increasing physical activity | Promotion of physical activityLeisure vs utilitarian physical activity |
| Unhealthy dietary patterns | Food environment:Making fruits and vegetables more available and less expensiveReducing the availability and increasing the prices of high-energy foodsImproving school cafeterias | Primary care programs and units for improving dietary quality | Nutritional health education programs in television programs and schools |
| Biological risk factors(Obesity, Cholesterol, Diabetes, Hypertension) | Campaigns for risk factors awareness and control * National salt reduction * | Creating primary care units with multidisciplinary teams to prevent and control body weight, lipids levels, glucose levels, and BP | Nutritional educationPhysical activity programsDevelopment of home BP monitoring programs |
BP, blood pressure; CVD, cardiovascular disease.
* See the above interventions for physical activity and diet.
In order to develop such policies, prevention efforts must be informed by a well developed monitoring system that would let us determine the distribution of relevant CHD risk factors, allowing preventive measures to be both adequate and comprehensive.10 Models such as IMPACT need to be informed by a network that gathers data in a valid and representative way and is able to picture the surveyed region taking into account social, economic, and health differences. Current monitoring systems have helped us determine and explain the causes of previous decreases in CHD mortality.14, 15
In summary, the informative results of applying the IMPACT model to the Spanish population help to confirm the ongoing importance of population-wide risk factor improvements and the appropriate delivery of evidence-based therapies, highlighting the considerable differences in the distribution of risk factors between men and women and the need for strategies to control smoking, obesity, and diabetes, factors which are impeding the overall downward CHD mortality trend in Spain.
CONFLICT OF INTERESTNone declared.
Corresponding author: Departamento de Epidemiología, Aterotrombosis e Imagen, Centro Nacional de Investigaciones Cardiovasculares (CNIC), Melchor Fernandez Almagro 3, 28029 Madrid, Spain. mfranco@cnic.es