Several errors were detected in the English translation of table 3 of the article “Coronavirus: the geriatric emergency of 2020. Joint document of the Section on Geriatric Cardiology of the Spanish Society of Cardiology and the Spanish Society of Geriatrics and Gerontology”. The correct table is:
Table 3.
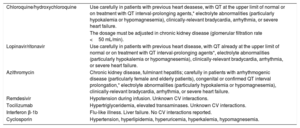
Adverse cardiovascular effects of drugs investigated for COVID-19 treatment
| Chloroquine/hydroxychloroquine | Use carefully in patients with previous heart deasese, with QT at the upper limit of normal or on treatment with QT interval-prolonging agents,* electrolyte abnormalities (particularly hypokalemia or hypomagnesemia), clinically-relevant bradycardia, arrhythmia, or severe heart failure. |
| The dosage must be adjusted in chronic kidney disease (glomerular filtration rate <50 mL/min). | |
| Lopinavir/ritonavir | Use carefully in patients with previous heart disease, with QT already at the upper limit of normal or on treatment with QT interval-prolonging agents*, electrolyte abnormalities (particularly hypokalemia or hypomagnesemia), clinically-relevant bradycardia, arrhythmia, or severe heart failure. |
| Azithromycin | Chronic kidney disease, fulminant hepatitis; carefully in patients with arrhythmogenic disease (particularly female and elderly patients), congenital or confirmed QT interval prolongation,* electrolyte abnormalities (particularly hypokalemia or hypomagnesemia), clinically-relevant bradycardia, arrhythmia, or severe heart failure. |
| Remdesivir | Hypotension during infusion. Unknown CV interactions. |
| Tocilizumab | Hypertriglyceridemia, elevated transaminases. Unknown CV interactions. |
| Interferon β-1b | Flu-like illness. Liver failure. No CV interactions reported. |
| Cyclosporin | Hypertension, hyperlipidemia, hyperuricemia, hyperkalemia, hypomagnesemia. |
CV, cardiovascular.
This correction has been made in the electronic version of the article on 12 October.
Copyright ©
2020. Sociedad Española de Cardiología