
A key priority of the Cardiovascular Health Strategy of the Spanish National Health System is improved understanding of the epidemiological and clinical reality of both health and cardiovascular disease, as well as its management. This information serves as a necessary starting point for any rational initiative for prevention and improvement. Recommendations for enhancing understanding include maximizing the use of information systems.1 In an article recently published in Revista Española de Cardiología, Camps-Vilaró et al.2 report the latest findings of a classic of Spanish cardiovascular epidemiological research, the REGICOR study. The results reveal significant improvements in Girona in both the incidence and lethality of acute myocardial infarction (AMI) in individuals < 75 years old in the last 3 decades (1990-2019). This study is doubly relevant, because of the value of the data reported and the method used. An additional aspect that should go without saying is that the data were segregated by sex. Although this should be the norm for all health data, as stressed by the Cardiovascular Health Strategy of the Spanish National Health System, it is not, which entails the extrapolation to women of results primarily obtained in men. This practice is incorrect, as confirmed in this study.
Although Girona already had one of the lowest incidences of AMI in developed countries (310 and 76 cases/100 000 men and women, respectively, in 1990-1994), the incidence has fallen by between 20% and 25% in both sexes. This represents annual reductions in absolute risk of 4.2% in men and 1% in women. These overall positive results can be attributed to various factors. The first factors comprise improvements both in population-level health promotion through education and lifestyle changes (less smoking, improved dietary patterns, and increased physical activity) and in secondary prevention measures. These achievements are primarily due to health and education authorities, for implementing policies in key areas, such as the banning of smoking in enclosed public spaces and laws favoring reductions in harmful foodstuffs or their accessibility in the most vulnerable populations (eg, children and adolescents), and due to primary care professionals, for their critical role in promoting health care and helping to prevent cardiovascular disease.
AMI lethality fell from almost 50% in 1990 to 1994 to 18% in the latest 5-year period, with a larger absolute reduction in annual risk in women than in men. Even after allowing for the possible influence of the changed definition of AMI on this reduction, particularly due to the use of high-sensitivity troponin, the results are still highly positive. The greater decrease in lethality has primarily been due to improvements in prehospital mortality (more marked, by the way, in women than in men), with smaller reductions in in-hospital mortality, which improved more modestly in women than in men. These advances can largely be explained by the following: greater population awareness of the need to rapidly notify emergency health care services in the presence of AMI-compatible symptoms, especially in women, which was the subject of a specific campaign in Catalonia; improvements in emergency care, both for out-of-hospital cardiac arrest associated with AMI and for the coordination of AMI care networks (Codi Infart in Catalonia); advances in the early management of AMI, such as reperfusion and adjunctive therapies; and improvements in their implementation.
However, we cannot become complacent. The flattening of the incidence and lethality curves is a sign that work remains to be done. Indeed, not only did the incidence in women aged between 65 and 74 years not decrease but it actually increased in the observation period, perhaps as a consequence of the increase in smoking in women of that generation, among other causes. Other population changes will have to monitored, such as the progressive aging of the population and lifestyle changes, because they could reverse or are even already reversing the favorable trends. Although population aging would not explain the findings of this “young” population in Girona, it is a threat that must be monitored and combated. Other worrisome trends include the falling adherence to the Mediterranean diet in Western societies3,4 and the increases in childhood obesity and, consequently, the future prevalence of diabetes mellitus.
The changes in lethality must also be carefully analyzed to identify areas for intervention. For example, in absolute terms, the lethality reductions have mainly occurred in the prehospital phase; however, this not only remains the largest contributor to lethality, but also has increased most in relative terms, rising from 2 out of every 3 deaths 3 decades ago to 3 out of every 4 deaths nowadays. This change, together with the marked improvement in in-hospital lethality, which had less room for maneuver, indicates 2 priorities: first, continued efforts to reduce prehospital lethality through population-wide educational campaigns (eg, the teaching of cardiopulmonary resuscitation in schools and workplaces and to public employees); and second, optimization of the functioning and coordination of emergency services, which have already been greatly improved.
The methodological aspects of this study are also important. As explained in the opening paragraph, problems surround the integration of AMI incidence and postdischarge mortality data.2 This situation has compromised the performance of epidemiological studies due to the difficulty of connecting clinical/administrative databases, such as the minimum data set, to mortality records based on death certificates. The present study addresses this problem by integrating both databases for the area of Girona using a specific linked data method. In addition, this integrated data set was validated using the results obtained in the previous REGICOR population registry, which provided comparable results. Finally, the authors use appropriate statistical techniques to evaluate changes in trends (joinpoint models). These techniques are particularly appropriate when data from different sources are used or when changes have been made to the registry or patient coding.
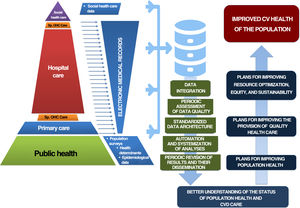
Technological advances can be used to more efficiently perform epidemiological studies by improving the data quality, particularly that of data obtained from electronic medical records. The current study is a good example of how to obtain comparable results after the transition from a population-based registry to clinical/administrative databases, such as the minimum data set, or to mortality registries. These databases need to be integrated for comparisons with more advanced countries in terms of clinical and epidemiological research.5-7 However, this integration is not a panacea and must be accompanied by a general improvement in the quality of the available data. This improvement must be centered on optimizing the architecture of the health care system data, performing systematic and periodic assessments of the quality of these data, and encouraging the integration of different data sources, ideally automatically, as indicated in the Cardiovascular Health Strategy of the Spanish National Health System.1 Regarding this last point, it is essential to increase the intercommunication between the primary care and hospital information systems and with other public administrative databases, such as population surveys and occupation or salary registries, given the prime importance of socioeconomic factors in the development of epidemiological research (figure 1).

The integration of the available data sources for the assessment and monitoring of population health status and of the management of cardiovascular disease, as well as the automation of their use and analysis, and the periodic and systematic reporting of the relevant information, should be a priority for public administrations and the Spanish National Health System. The REGICOR study used this approach to reveal the worrying stabilization in the fall in AMI incidence and lethality in Girona and proves the need for further investment in primary and secondary prevention strategies for AMI prevention, because these are the most reasonable and cost-effective approaches and those that can provide a greater incremental benefit compared with strategies focused on acute care.
FUNDINGThe present editorial has not received funding.
CONFLICTS OF INTERESTNo conflicts of interest are reported in relation to this article. N. Rosillo receives funding from a Río Hortega contract (CM22/00049). H. Bueno receives research funding from the Instituto de Salud Carlos III (PI21/01572), the Spanish Society of Cardiology, AstraZeneca, Janssen, and Novartis and has received payments for consulting and conferences from AstraZeneca, Novartis, Novo Nordisk, and Organon.