
Acute coronary syndromes are a leading cause of mortality, morbidity, and health care cost in Spain. The aims of this report are to estimate the number of acute coronary syndromes cases in the Spanish population in 2013 and 2021, and the trend from 2005 to 2049. We estimated the number of acute coronary syndromes cases by sex and Spanish autonomous community using data from the most updated population and hospital registries. We present the estimated number of cases with an exact 95% confidence interval, assuming that the number of cases followed a Poisson distribution. There will be 115 752 acute coronary syndromes cases in Spain in 2013 (95% confidence interval, 114 822-116 687). Within 28 days, 39 086 of these patients will die and 85 326 will be hospitalized. Non-ST segment elevation acute coronary syndromes (56%) and acute myocardial infarction (81%) will be the most common admission and discharge diagnoses, respectively. We estimate approximately 109 772 acute coronary syndromes cases in 2021 (95% confidence interval, 108 868-110 635). The trend of acute coronary syndromes cases from 2005 to 2049 will stabilize in the population aged 25 to 74 years, but increase in those older than 74 years. Due to population aging, the number of acute coronary syndrome cases will increase overall until 2049, it may stabilize in the population aged <75 years. The acute coronary syndromes case-fatality has decreased in hospitalized patients but the proportion of sudden deaths remains unchanged.
Keywords
.
In the present European and worldwide context of high rates of mortality attributed to cardiovascular diseases, and given their great impact on the population and the economic burden on our society, throughout 2013 the Revista Española de Cardiología will publish, in its “Focus on” section, four chapters under the title “Epidemiology of Cardiovascular Disease in Spain Over the Past 20 Years”. This series proposes an updated review of the epidemiological data on four cardiovascular diseases that, for one reason or another (in general, because of their high prevalence), have great impact on the health of the Spanish population: ischemic heart disease, heart failure, atrial fibrillation, and infective endocarditis.
Coronary artery disease (CAD) has been the single leading cause of death in the Spanish population for over 30 years, and acute coronary syndromes (ACS) are a leading cause of mortality, morbidity, and health care cost in Spain.
During this same period mortality due to this disease has declined, mainly because of a decrease in deaths among patients who arrive to a hospital for treatment. This decline in mortality while incidence appears to remain stable has led to an increased prevalence of CAD and its complications, one of which is heart failure. The incidence of heart failure has also increased due to the aging of the population, which in turn has led to an increased incidence of atrial fibrillation, an arrhythmia responsible for a large proportion of cardiology and primary care consultations. Finally, in this “Focus On” section, we will deal with a problem that is less common but still poses many health care concerns and uncertainties: infective endocarditis.
INTRODUCTIONACS are the most common and deleterious clinical manifestation of CAD,1,2 which continues to be the leading cause of death and morbidity in Europe, although the disease burden varies with latitude.3 ACS results in two main discharge diagnoses: unstable angina (UA) and acute myocardial infarction (AMI).
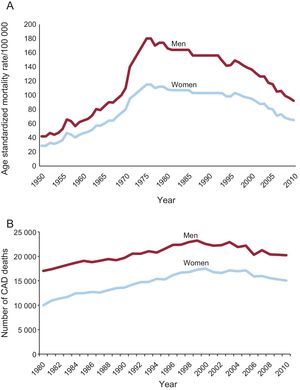
In Spain, CAD mortality rates have steadily decreased in the past 40 years (Fig. 1A). However, the absolute number of CAD deaths increased from 1980 to 2000 and steadily declined thereafter (Fig. 1B); CAD is still the first and the second most common individual cause of death in men and women, respectively.4

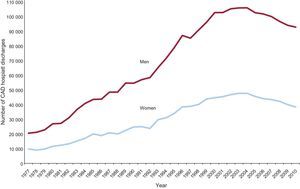
Concerning morbidity, Spanish AMI incidence rates remained relatively stable during the last 20 years of the past century, before the release of the 2000 AMI definition.5,6 CAD discharges increased from 31 032 in 1977 to 152 190 in 2004, and declined thereafter to 129 944 in 2010 (Fig. 2).7 The initial increase was probably caused in part by the new definition of AMI, by the increased elderly population with a higher ACS incidence rate than in younger age groups, and by improved survival after an acute coronary event, which increases the number of prevalent CAD patients, known to require subsequent readmissions.8–10 A new balance between the number of incident cases and CAD-survivors cohort mortality seems to have been reached after 2004, as mortality in the CAD cohort would have increased in recent years with the progressive aging of its members.

ACS care consumes a large amount of resources in Spain. At the beginning of the 21st century, direct health care costs alone were €1.03 billion annually for patients in the first year after diagnosis of ACS.11 In order to allocate human and economic resources appropriately it is essential to have data on the expected number of total and fatal cases of ACS as well as on readmissions for ACS, as it is known that the cost per patient increases with severity.12
In a previous study8 we estimated the projected number of AMI cases for 1997-2005 using the pre-2000 AMI definition, which included the use of troponine level to identify myocardial necrosis. New interest in quantifying the impact of the 2000 definition on the number of AMI cases in clinical practice and developing clinical interest in ACS prompt this update on the estimated number of ACS cases in Spain in the decades to come. The aims of this report are: a) to estimate the number of fatal and nonfatal ACS cases in 2013 and 2021, and b) to estimate the trend of ACS cases for the period 2005-2049. Our secondary aim was to analyze the number of hospitalized ACS cases by discharge diagnosis (ie, myocardial infarction and UA), which is related to prognosis, severity, and future events.
METHODSMost of the data sources for our estimations and analyses are based on descriptive studies of the ACS burden published in peer-reviewed journals in the past decade. We also used unpublished data from the REGICOR (REgistre GIroní del COR, which stands for Girona Heart Registry) study when no other source was available.13 The study projects the number of AMI and UA cases likely to occur in the population older than 24 years.
Estimation of the Total Number of Population and Hospitalized Acute Coronary Syndromes CasesTo calculate the number of ACS cases in the Spanish population and their 95% confidence intervals (95%CI), we used the following sources.
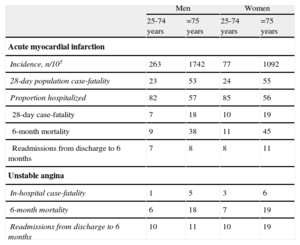
The number of AMI cases in the population was estimated using crude incidence rates and population estimates by decennial age groups (25-34; 35-44; 45-54, 55-64; 65-74; 75 or older) and sex. Crude incidence rates for the older group by sex were obtained from the REGICOR study (Table 1). Crude incidence rates for the other age groups were obtained from the IBERICA study (1997-1998),14 and corrected by the increase since 2000 that is due to the use of troponin determination in diagnosing AMI. This increase was calculated using findings from the REGICOR study by sex and age group (Table 1, footnote). Crude rates from the IBERICA study were available for the following Spanish autonomous communities: Balearic Islands, Castile-La Mancha, Catalonia, Region of Murcia, Chartered Community of Navarre and Basque Country. In the remaining autonomous communities we used the mean IBERICA crude rates.
Basic Data on Annual Incidence Rate, Case-fatality, 6-month Mortality and Readmissions After an Acute Myocardial Infarction or Unstable Angina Event Projected for 2013 in Spain
| Men | Women | |||
| 25-74 years | =75 years | 25-74 years | =75 years | |
| Acute myocardial infarction | ||||
| Incidence, n/105 | 263 | 1742 | 77 | 1092 |
| 28-day population case-fatality | 23 | 53 | 24 | 55 |
| Proportion hospitalized | 82 | 57 | 85 | 56 |
| 28-day case-fatality | 7 | 18 | 10 | 19 |
| 6-month mortality | 9 | 38 | 11 | 45 |
| Readmissions from discharge to 6 months | 7 | 8 | 8 | 11 |
| Unstable angina | ||||
| In-hospital case-fatality | 1 | 5 | 3 | 6 |
| 6-month mortality | 6 | 18 | 7 | 19 |
| Readmissions from discharge to 6 months | 10 | 11 | 10 | 19 |
Assumptions: Increase in the number of acute myocardial infarction events due to the use of troponin values in the diagnosis (according to the REGICOR study): 14% (men, 25-74 years); 50% (men, =75 years); 28% (women, 25-74 years); 64% (women, =75 years).
Unless otherwise indicated, data express percentage.
Population estimates and projections for the years 2013 and 2021 and to 2049 by autonomous community, decennial age group, and sex were obtained from the National Institute of Statistics (Instituto Nacional de Estadística, INE).15–17
To estimate the number of hospitalized AMI cases we calculated the hospitalization rate using REGICOR data, by sex and age group (Table 1). The proportion of ST elevation, non-ST elevation and nonclassifiable hospitalized ACS patients was that of the MASCARA study, as well as the proportion of AMI, UA and other discharge diagnoses of hospitalized ACS cases,18,19 by sex and age groups (Tables 2–4, footnote). We assumed that 100% of the UA cases were hospitalized. The calculated number of UA cases was added to the number of hospitalized and population AMI cases to obtain total hospitalized and population numbers of ACS cases.
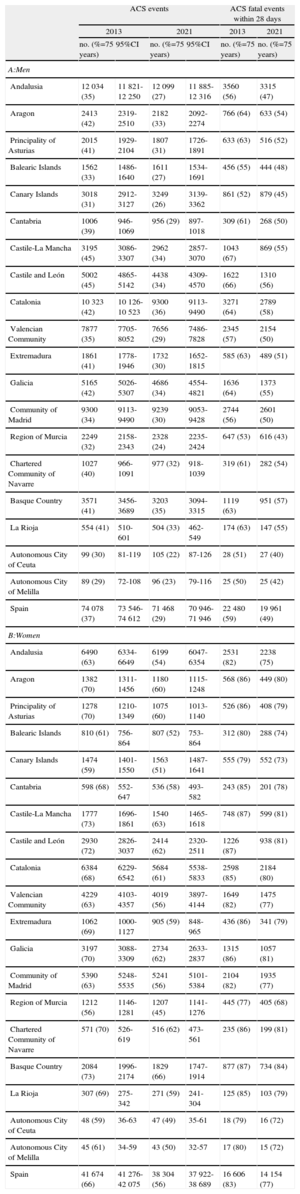
Number of Total and Fatal Acute Coronary Syndrome Event Estimation in Population Older Than 24 Years, by Year, Sex and Spanish Autonomous Community
| ACS events | ACS fatal events within 28 days | |||||
| 2013 | 2021 | 2013 | 2021 | |||
| no. (%=75 years) | 95%CI | no. (%=75 years) | 95%CI | no. (%=75 years) | no. (%=75 years) | |
| A:Men | ||||||
| Andalusia | 12 034 (35) | 11 821-12 250 | 12 099 (27) | 11 885-12 316 | 3560 (56) | 3315 (47) |
| Aragon | 2413 (42) | 2319-2510 | 2182 (33) | 2092-2274 | 766 (64) | 633 (54) |
| Principality of Asturias | 2015 (41) | 1929-2104 | 1807 (31) | 1726-1891 | 633 (63) | 516 (52) |
| Balearic Islands | 1562 (33) | 1486-1640 | 1611 (27) | 1534-1691 | 456 (55) | 444 (48) |
| Canary Islands | 3018 (31) | 2912-3127 | 3249 (26) | 3139-3362 | 861 (52) | 879 (45) |
| Cantabria | 1006 (39) | 946-1069 | 956 (29) | 897-1018 | 309 (61) | 268 (50) |
| Castile-La Mancha | 3195 (45) | 3086-3307 | 2962 (34) | 2857-3070 | 1043 (67) | 869 (55) |
| Castile and León | 5002 (45) | 4865-5142 | 4438 (34) | 4309-4570 | 1622 (66) | 1310 (56) |
| Catalonia | 10 323 (42) | 10 126-10 523 | 9300 (36) | 9113-9490 | 3271 (64) | 2789 (58) |
| Valencian Community | 7877 (35) | 7705-8052 | 7656 (29) | 7486-7828 | 2345 (57) | 2154 (50) |
| Extremadura | 1861 (41) | 1778-1946 | 1732 (30) | 1652-1815 | 585 (63) | 489 (51) |
| Galicia | 5165 (42) | 5026-5307 | 4686 (34) | 4554-4821 | 1636 (64) | 1373 (55) |
| Community of Madrid | 9300 (34) | 9113-9490 | 9239 (30) | 9053-9428 | 2744 (56) | 2601 (50) |
| Region of Murcia | 2249 (32) | 2158-2343 | 2328 (24) | 2235-2424 | 647 (53) | 616 (43) |
| Chartered Community of Navarre | 1027 (40) | 966-1091 | 977 (32) | 918-1039 | 319 (61) | 282 (54) |
| Basque Country | 3571 (41) | 3456-3689 | 3203 (35) | 3094-3315 | 1119 (63) | 951 (57) |
| La Rioja | 554 (41) | 510-601 | 504 (33) | 462-549 | 174 (63) | 147 (55) |
| Autonomous City of Ceuta | 99 (30) | 81-119 | 105 (22) | 87-126 | 28 (51) | 27 (40) |
| Autonomous City of Melilla | 89 (29) | 72-108 | 96 (23) | 79-116 | 25 (50) | 25 (42) |
| Spain | 74 078 (37) | 73 546-74 612 | 71 468 (29) | 70 946-71 946 | 22 480 (59) | 19 961 (49) |
| B:Women | ||||||
| Andalusia | 6490 (63) | 6334-6649 | 6199 (54) | 6047-6354 | 2531 (82) | 2238 (75) |
| Aragon | 1382 (70) | 1311-1456 | 1180 (60) | 1115-1248 | 568 (86) | 449 (80) |
| Principality of Asturias | 1278 (70) | 1210-1349 | 1075 (60) | 1013-1140 | 526 (86) | 408 (79) |
| Balearic Islands | 810 (61) | 756-864 | 807 (52) | 753-864 | 312 (80) | 288 (74) |
| Canary Islands | 1474 (59) | 1401-1550 | 1563 (51) | 1487-1641 | 555 (79) | 552 (73) |
| Cantabria | 598 (68) | 552-647 | 536 (58) | 493-582 | 243 (85) | 201 (78) |
| Castile-La Mancha | 1777 (73) | 1696-1861 | 1540 (63) | 1465-1618 | 748 (87) | 599 (81) |
| Castile and León | 2930 (72) | 2826-3037 | 2414 (62) | 2320-2511 | 1226 (87) | 938 (81) |
| Catalonia | 6384 (68) | 6229-6542 | 5684 (61) | 5538-5833 | 2598 (85) | 2184 (80) |
| Valencian Community | 4229 (63) | 4103-4357 | 4019 (56) | 3897-4144 | 1649 (82) | 1475 (77) |
| Extremadura | 1062 (69) | 1000-1127 | 905 (59) | 848-965 | 436 (86) | 341 (79) |
| Galicia | 3197 (70) | 3088-3309 | 2734 (62) | 2633-2837 | 1315 (86) | 1057 (81) |
| Community of Madrid | 5390 (63) | 5248-5535 | 5241 (56) | 5101-5384 | 2104 (82) | 1935 (77) |
| Region of Murcia | 1212 (56) | 1146-1281 | 1207 (45) | 1141-1276 | 445 (77) | 405 (68) |
| Chartered Community of Navarre | 571 (70) | 526-619 | 516 (62) | 473-561 | 235 (86) | 199 (81) |
| Basque Country | 2084 (73) | 1996-2174 | 1829 (66) | 1747-1914 | 877 (87) | 734 (84) |
| La Rioja | 307 (69) | 275-342 | 271 (59) | 241-304 | 125 (85) | 103 (79) |
| Autonomous City of Ceuta | 48 (59) | 36-63 | 47 (49) | 35-61 | 18 (79) | 16 (72) |
| Autonomous City of Melilla | 45 (61) | 34-59 | 43 (50) | 32-57 | 17 (80) | 15 (72) |
| Spain | 41 674 (66) | 41 276-42 075 | 38 304 (56) | 37 922-38 689 | 16 606 (83) | 14 154 (77) |
95%CI, 95% confidence interval; ACS, acute coronary syndromes.
Assumptions: 100% of the unstable angina cases were hospitalized.
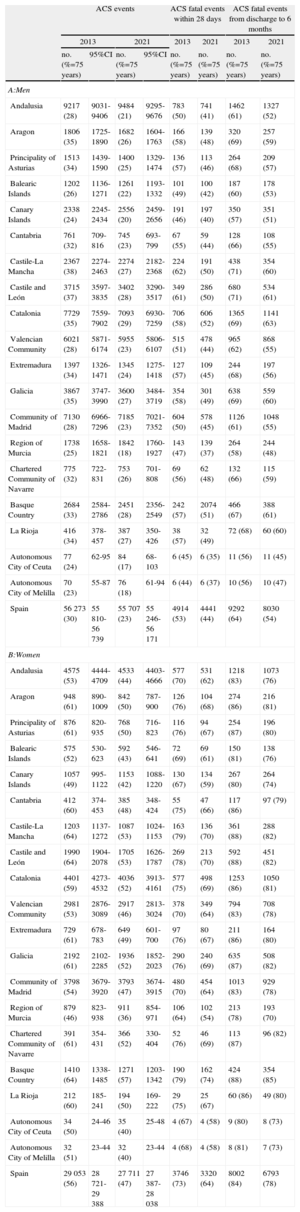
Number of Total and Fatal Acute Coronary Syndrome Hospitalized Patients Older Than 24 Years, Estimated by Year, Sex and Spanish Autonomous Community
| ACS events | ACS fatal events within 28 days | ACS fatal events from discharge to 6 months | ||||||
| 2013 | 2021 | 2013 | 2021 | 2013 | 2021 | |||
| no. (%=75 years) | 95%CI | no. (%=75 years) | 95%CI | no. (%=75 years) | no. (%=75 years) | no. (%=75 years) | no. (%=75 years) | |
| A:Men | ||||||||
| Andalusia | 9217 (28) | 9031-9406 | 9484 (21) | 9295-9676 | 783 (50) | 741 (41) | 1462 (61) | 1327 (52) |
| Aragon | 1806 (35) | 1725-1890 | 1682 (26) | 1604-1763 | 166 (58) | 139 (48) | 320 (69) | 257 (59) |
| Principality of Asturias | 1513 (34) | 1439-1590 | 1400 (25) | 1329-1474 | 136 (57) | 113 (46) | 264 (68) | 209 (57) |
| Balearic Islands | 1202 (26) | 1136-1271 | 1261 (22) | 1193-1332 | 101 (49) | 100 (42) | 187 (60) | 178 (53) |
| Canary Islands | 2338 (24) | 2245-2434 | 2556 (20) | 2459-2656 | 191 (46) | 197 (40) | 350 (57) | 351 (51) |
| Cantabria | 761 (32) | 709-816 | 745 (23) | 693-799 | 67 (55) | 59 (44) | 128 (66) | 108 (55) |
| Castile-La Mancha | 2367 (38) | 2274-2463 | 2274 (27) | 2182-2368 | 224 (62) | 191 (50) | 438 (71) | 354 (60) |
| Castile and León | 3715 (37) | 3597-3835 | 3402 (28) | 3290-3517 | 349 (61) | 286 (50) | 680 (71) | 534 (61) |
| Catalonia | 7729 (35) | 7559-7902 | 7093 (29) | 6930-7259 | 706 (58) | 606 (52) | 1365 (69) | 1141 (63) |
| Valencian Community | 6021 (28) | 5871-6174 | 5955 (23) | 5806-6107 | 515 (51) | 478 (44) | 965 (62) | 868 (55) |
| Extremadura | 1397 (34) | 1326-1471 | 1345 (24) | 1275-1418 | 127 (57) | 109 (45) | 244 (68) | 197 (56) |
| Galicia | 3867 (35) | 3747-3990 | 3600 (27) | 3484-3719 | 354 (58) | 301 (49) | 638 (69) | 559 (60) |
| Community of Madrid | 7130 (28) | 6966-7296 | 7185 (23) | 7021-7352 | 604 (50) | 578 (45) | 1126 (61) | 1048 (55) |
| Region of Murcia | 1738 (25) | 1658-1821 | 1842 (18) | 1760-1927 | 143 (47) | 139 (37) | 264 (58) | 244 (48) |
| Chartered Community of Navarre | 775 (32) | 722-831 | 753 (26) | 701-808 | 69 (56) | 62 (48) | 132 (66) | 115 (59) |
| Basque Country | 2684 (33) | 2584-2786 | 2451 (28) | 2356-2549 | 242 (57) | 2074 (51) | 466 (67) | 388 (61) |
| La Rioja | 416 (34) | 378-457 | 387 (27) | 350-426 | 38 (57) | 32 (49) | 72 (68) | 60 (60) |
| Autonomous City of Ceuta | 77 (24) | 62-95 | 84 (17) | 68-103 | 6 (45) | 6 (35) | 11 (56) | 11 (45) |
| Autonomous City of Melilla | 70 (23) | 55-87 | 76 (18) | 61-94 | 6 (44) | 6 (37) | 10 (56) | 10 (47) |
| Spain | 56 273 (30) | 55 810-56 739 | 55 707 (23) | 55 246-56 171 | 4914 (53) | 4441 (44) | 9292 (64) | 8030 (54) |
| B:Women | ||||||||
| Andalusia | 4575 (53) | 4444-4709 | 4533 (44) | 4403-4666 | 577 (70) | 531 (62) | 1218 (83) | 1073 (76) |
| Aragon | 948 (61) | 890-1009 | 842 (50) | 787-900 | 126 (76) | 104 (68) | 274 (86) | 216 (81) |
| Principality of Asturias | 876 (61) | 820-935 | 768 (50) | 716-823 | 116 (76) | 94 (67) | 254 (87) | 196 (80) |
| Balearic Islands | 575 (52) | 530-623 | 592 (43) | 546-641 | 72 (69) | 69 (61) | 150 (81) | 138 (76) |
| Canary Islands | 1057 (49) | 995-1122 | 1153 (42) | 1088-1220 | 130 (67) | 134 (59) | 267 (80) | 264 (74) |
| Cantabria | 412 (60) | 374-453 | 385 (48) | 348-424 | 55 (75) | 47 (66) | 117 (86) | 97 (79) |
| Castile-La Mancha | 1203 (64) | 1137-1272 | 1087 (53) | 1024-1153 | 163 (79) | 136 (70) | 361 (88) | 288 (82) |
| Castile and León | 1990 (64) | 1904-2078 | 1705 (53) | 1626-1787 | 269 (78) | 213 (70) | 592 (88) | 451 (82) |
| Catalonia | 4401 (59) | 4273-4532 | 4036 (52) | 3913-4161 | 577 (75) | 498 (69) | 1253 (86) | 1050 (81) |
| Valencian Community | 2981 (53) | 2876-3089 | 2917 (46) | 2813-3024 | 378 (70) | 349 (64) | 794 (83) | 708 (78) |
| Extremadura | 729 (61) | 678-783 | 649 (49) | 601-700 | 97 (76) | 80 (67) | 211 (86) | 164 (80) |
| Galicia | 2192 (61) | 2102-2285 | 1936 (52) | 1852-2023 | 290 (76) | 240 (69) | 635 (87) | 508 (82) |
| Community of Madrid | 3798 (54) | 3679-3920 | 3793 (47) | 3674-3915 | 480 (70) | 454 (64) | 1013 (83) | 929 (78) |
| Region of Murcia | 879 (46) | 823-938 | 911 (36) | 854-971 | 106 (64) | 102 (54) | 213 (78) | 193 (70) |
| Chartered Community of Navarre | 391 (61) | 354-431 | 366 (52) | 330-404 | 52 (76) | 46 (69) | 113 (87) | 96 (82) |
| Basque Country | 1410 (64) | 1338-1485 | 1271 (57) | 1203-1342 | 190 (79) | 162 (74) | 424 (88) | 354 (85) |
| La Rioja | 212 (60) | 185-241 | 194 (50) | 169-222 | 29 (75) | 25 (67) | 60 (86) | 49 (80) |
| Autonomous City of Ceuta | 34 (50) | 24-46 | 35 (40) | 25-48 | 4 (67) | 4 (58) | 9 (80) | 8 (73) |
| Autonomous City of Melilla | 32 (51) | 23-44 | 32 (40) | 23-44 | 4 (68) | 4 (58) | 8 (81) | 7 (73) |
| Spain | 29 053 (56) | 28 721-29 388 | 27 711 (47) | 27 387-28 038 | 3746 (73) | 3320 (64) | 8002 (84) | 6793 (78) |
95%CI, 95% confidence interval; ACS, acute coronary syndromes.
Assumptions: Contribution of unstable angina to hospitalized ACS cases (proportion obtained from MASCARA data): 25% (women, 25-74 years); 15% (women, =75 years); 18% (men, 25-74 years and >74 years).
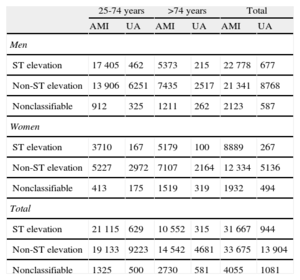
Estimated Distribution of the 85 326 Hospitalized Acute Coronary Syndrome Cases in 2013 in the Spanish Population Older Than 24 Years, by Admission and Discharge Diagnosis, Sex and Age Group
| 25-74 years | >74 years | Total | ||||
| AMI | UA | AMI | UA | AMI | UA | |
| Men | ||||||
| ST elevation | 17 405 | 462 | 5373 | 215 | 22 778 | 677 |
| Non-ST elevation | 13 906 | 6251 | 7435 | 2517 | 21 341 | 8768 |
| Nonclassifiable | 912 | 325 | 1211 | 262 | 2123 | 587 |
| Women | ||||||
| ST elevation | 3710 | 167 | 5179 | 100 | 8889 | 267 |
| Non-ST elevation | 5227 | 2972 | 7107 | 2164 | 12 334 | 5136 |
| Nonclassifiable | 413 | 175 | 1519 | 319 | 1932 | 494 |
| Total | ||||||
| ST elevation | 21 115 | 629 | 10 552 | 315 | 31 667 | 944 |
| Non-ST elevation | 19 133 | 9223 | 14 542 | 4681 | 33 675 | 13 904 |
| Nonclassifiable | 1325 | 500 | 2730 | 581 | 4055 | 1081 |
AMI, acute myocardial infarction; UA, unstable angina.
Assumptions: percentage of cases by discharge diagnosis, age and sex group taken from the MASCARA study.
The number of fatal ACS cases in the Spanish population was calculated using 28-day AMI case-fatality and in-hospital UA case-fatality, by sex and age group, under the assumption that all pre-hospital deaths were AMI cases. The population 28-day AMI case-fatality was obtained from the REGICOR study (Table 1). The number of hospitalized ACS cases estimated to be 28-day and 6-month fatalities was calculated using hospitalized AMI and UA cases. The 28-day case-fatality for hospitalized AMI was calculated using REGICOR data by sex and age group, and in-hospital UA case-fatality and 6-month mortality and readmission for discharged AMI and UA patients were obtained from the MASCARA study (Table 1).18
Estimation of the Hospitalized Number of Acute Coronary Syndromes Cases by Admission and Discharge DiagnosisThe number of hospitalized cases expected in 2013 according to the admission diagnosis (ST elevation, non-ST elevation, nonclassifiable) and discharge diagnosis (AMI, UA) was calculated using the percentage of cases of each diagnosis by sex and age group from the MASCARA study.18 The starting point was the estimated number of hospitalized ACS cases by sex and age group.
Estimation of the Population 2005-2049 Trend in the Number of Acute Coronary SyndromesThe 2005-2049 annual number of population ACS cases by sex and age group was obtained by projecting to 2020 the 1990-2009 trends in annual AMI incidence rate for two age groups (25-74 years and =75 years) observed in the REGICOR study, assuming that the incidence rate would remain stable thereafter, and using population estimates or projections by sex and age group provided by the INE.15–17
ValidationTo validate our estimates we calculated the ratio of estimated to official cases for hospitalized AMI and population fatal CAD. We estimated the number of hospitalized AMI cases and population fatal CAD cases as described in the 2010 population estimates, the most recent official statistics on CAD mortality and AMI hospitalization available from the INE.4,7 We note here that Figure 2 is derived from the number of hospitalized patients with any type of CAD rather than AMI alone.
Statistical AnalysisExact 95%CI were calculated for the number of population and hospitalized ACS cases by Spanish autonomous community, assuming that the number of cases followed a Poisson distribution. Analyses were performed using version 2.14.2 of the R statistical program (R Development Core Team,).
RESULTSBasic Spanish data on incidence, case-fatality, 6-month mortality and readmissions for AMI and UA by sex and age groups are summarized in Table 1. AMI incidence rate was higher in men than in women in all age groups. However, population 28-day case-fatality and 6-month mortality in hospitalized AMI was higher in women than in men for both age groups. The readmission rate in the first 6 months after discharge was around 8% for all sex and age groups except women older than 74 years, in whom it reaches 11%. There were 4 times as many deaths in the over-74 population as in the younger age group. Regarding UA, there are more deaths within the first 28 days in women than in men. The 6-month readmission rate is higher in women older than 74 years (19%) than in the other groups (around 10%). From discharge to 6 months, deaths are 3 times more likely in the older age group than in the younger population.
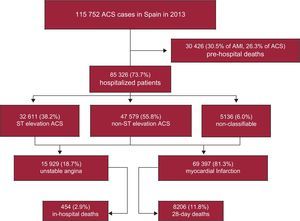
Table 2 shows the estimated total number and estimated fatal ACS cases (AMI and UA) in the Spanish population by sex and autonomous community in 2013 and 2021. Similar estimates for hospitalized cases are also depicted by sex in Table 3. We have estimated that there will be 115 752 ACS cases in Spain in 2013 (95%CI: 114 822-116 687), 74 078 in men and 41 674 in women (Tables 2A and B); 28-day mortality is projected to be 39086 (33.8%). From the total number of ACS cases, 99 823 (86.2%) will be AMI cases and 38 633 of them (38.7%) will die within the first 28 days. From a clinical perspective, 85 326 (95%CI: 84 531-86 127) will be hospitalized (73.7%); 69 397 (81.3%) will be AMI and 15 929 UA cases. Of these patients, 8660 (10.2%) will die within 28 days of admission (Tables 3A and B; Fig. 3). Among the 76 666 ACS survivors, 8420 patients (7193 AMI and 1227 UA) will die within 6 months after discharge (11.0%).

In men, 37% of the total ACS cases and 59% of the fatal ACS cases in 2013 will occur in patients older than 75 years. In women, 66% of the total population ACS cases and 83% of the fatal ACS cases will occur in the older group (Tables 2A and B). Among hospitalized ACS cases, the older age group will represent 30% of the total ACS cases and 53% of the fatal ACS cases in men. In women, the older age group will represent 56% of the total ACS cases and 73% of the fatal ACS cases (Tables 3A and B).
With respect to ACS cases by autonomous community, in 2013 Andalusia will be the Spanish region contributing the highest number of ACS cases in both men and women (Tables 2A and B). By age group, Andalusia will contribute the most ACS cases in the population aged 25 to 74 years, while Catalonia will contribute the most cases in the over-74 population. Four communities (Andalusia, Catalonia, Valencian Community and Community of Madrid) will contribute more than 50% of total and fatal ACS cases, both at a population and hospitalized level.
Assuming that the observed 1990-2009 trends in AMI incidence and 28-day case-fatality rates for both age groups (Table 1) will continue until 2020 and both rates will be stable thereafter, we anticipate 109 772 (95%CI: 108 868-110 635) ACS cases by 2021 in Spain, with a 28-day mortality of 31.1% (34 115 deaths). Of the 83 418 (76.0%) patients who will reach the hospital, both 28-day and 6-month mortality will be just 9.3% (7761 and 7062 deaths, respectively) (Table 3).
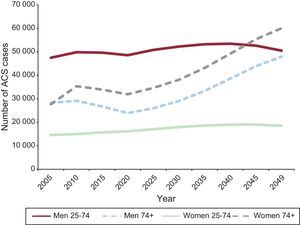
Moreover, we estimate an important increase in the number of ACS cases in Spain over the next 35 to 40 years (Fig. 4) as the population aged 75 years or older reaches 24% of the total Spanish population by 2049. From 2013 to 2049 ACS cases will increase 69% to 116% in the older age group, rising from 28 296 to 47 920 in men and from 27 651 to 59 990 in women. On the other hand, the cases contributed by those aged 25 to 74 years will increase by 6% in men and by 26% in women if our assumptions about population trends and projections are correct.

Analysis of clinical diagnosis records indicates that 38.2% of all 2013 ACS cases will be categorized as ST elevation at admission, 55.8% as non-ST elevation and 6.0% as nonclassifiable (Table 4). We estimate that non-ST segment elevation ACS will be the most common diagnosis at admission, accounting for 53.5% and 60.1% of the cases in men and women, respectively. It also will be the most common diagnosis in all age groups analyzed. At discharge, we expect 81.3% of all 2013 ACS cases to be diagnosed as AMI and 18.7% as UA. In the MASCARA study, 9% of the initially suspected ACS cases received other diagnoses at discharge, such as stable angina or chest pain of nonischemic heart disease origin. This would increase the burden of hospital care by some 8439 ACS-suspected patients in 2013. The percentage of ACS cases discharged as AMI will be similar in men (82.2%) and women (79.7%) and in both age groups: 25 to 74 years (80.1%) and 75 years or older (83.3%).
The ratio for 2010 between our estimate and the official number of hospitalized AMI cases in Spain was 1.27, and between our estimate and the official number of CAD fatal cases was 1.12. Table 5 shows these ratios by autonomous community.
Estimated and Official Number of Hospitalized Acute Myocardial Infarction Patients and of Fatal Coronary Artery Disease Events in 2010 in Population Older Than 24 Years, by Spanish Autonomous Community
| Hospitalized AMI events | Fatal CAD events | |||||
| Estimated | Official | Ratio | Estimated | Official | Ratio | |
| Andalusia | 11 190 | 9994 | 1.12 | 6077 | 6706 | 0.91 |
| Aragon | 2331 | 1448 | 1.61 | 1388 | 1061 | 1.31 |
| Principality of Asturias | 2026 | 1572 | 1.29 | 1208 | 1368 | 0.88 |
| Balearic Islands | 1424 | 1196 | 1.19 | 758 | 700 | 1.08 |
| Canary Islands | 2658 | 2376 | 1.12 | 1352 | 1332 | 1.02 |
| Cantabria | 973 | 749 | 1.30 | 566 | 406 | 1.39 |
| Castile-La Mancha | 4865 | 3581 | 1.36 | 2975 | 2454 | 1.21 |
| Castile and León | 3001 | 2593 | 1.16 | 1846 | 1594 | 1.16 |
| Catalonia | 10 099 | 8166 | 1.24 | 5953 | 4780 | 1.25 |
| Valencian Community | 7343 | 6170 | 1.19 | 3986 | 4328 | 0.92 |
| Extremadura | 1792 | 1387 | 1.29 | 1057 | 1010 | 1.05 |
| Galicia | 5093 | 3305 | 1.54 | 3021 | 2574 | 1.17 |
| Community of Madrid | 8798 | 6381 | 1.38 | 4755 | 3560 | 1.34 |
| Region of Murcia | 2092 | 1846 | 1.13 | 1076 | 888 | 1.21 |
| Chartered Community of Navarre | 965 | 638 | 1.51 | 563 | 346 | 1.63 |
| Basque Country | 3423 | 2258 | 1.52 | 2020 | 1474 | 1.37 |
| La Rioja | 526 | 363 | 1.45 | 307 | 213 | 1.44 |
| Autonomous City of Ceuta | 89 | 73 | 1.22 | 45 | 40 | 1.13 |
| Autonomous City of Melilla | 81 | 67 | 1.21 | 42 | 41 | 1.01 |
| Spain | 68 769 | 54 163 | 1.27 | 38 995 | 34 875 | 1.12 |
AMI, acute myocardial infarction; CAD, coronary artery disease.
We estimate that the number of population and hospitalized ACS cases in Spain in 2013 will be 115 752 and 85 326, respectively. In a previously published estimate8 these figures were 102 023 and 74 518, respectively, and AMI diagnoses constituted 67% and 55% of these cases, respectively. In the current estimation the AMI figures have increased to 87% of population cases and 82% of hospitalized ACS patients. This change is mostly related to the increasing use and sensitivity of troponins since 2000, when the ACS definition was revised. Most of the 74 078 ACS cases in Spanish men will occur in the population aged 25 to 74 years, while in women the majority of the 41 674 cases will occur in those aged 75 years or more.
In 2013, 28-day ACS mortality will be 34% overall, 10% in patients arriving alive at the hospital and 26% in out-of-hospital deaths. These figures are slightly improved, particularly for hospitalized patients, over the 2002 estimates of 38%, 15%, and 27%, respectively.8
When considering only AMI, the population and hospitalized patients case-fatality decline is in large part related to the revision of the AMI definition in 2000.20–24 However, a significant reduction of approximately 30% to 40% in crude AMI in-hospital case-fatality has also been described in a similar time period in Spain as a whole, Ireland, United States, and Canada.19,25–27 Moreover, a longer period of observation shows that since 1995 there has been a 30% to 50% decrease in AMI population case-fatality and 50% to 60% decrease in AMI in-hospital case fatality.8 All these data concur with the estimated 33% reduction in hospitalized ACS 28-day case fatality.
We did not observe a significant reduction in out-of-hospital case-fatality between our earlier and current calculations. It has been suggested that a decrease in out-of-hospital mortality may be related to primary prevention, while in-hospital mortality may decrease as a result of improved medical care, such as extended use of effective drugs or percutaneous coronary intervention.19,28 Thus, the large decrease in AMI case-fatality observed would be mostly due to advances in acute medical care, as previously reported.29 More attention and effort should be directed toward primary prevention of the disease.
According to the MASCARA study results we assumed that non-ST elevation ACS (NSTEACS) is the main admission diagnosis for ACS while the most common discharge diagnosis will be AMI.18 Data from other studies also indicate that NSTEACS is the most frequent cause of ACS hospitalization but ACS clinical and anatomical patterns differ for ST segment elevation.24,30–34 In recent years, the proportion of patients with ST segment elevation ACS (STEACS) has decreased while the proportion of NSTEACS patients has increased. Patients with NSTEACS tend to be older and have more extensive CAD.31 Thus, taking into account the predicted aging of the population we expect an increase in the percentage of NSTEACS patients in the coming decades. Our trend analysis shows that the number of ACS cases will slightly decrease to 109 772 in 2021 but will increase to 175 751 in 2049 due to the aging of the population. During the last 10 years the Spanish population aged 25 to 74 years has increased by 15% while the population aged 75 years or more has increased by 34%.15 Moreover, it is expected that from 2013 to 2049, those aged 25 to 74 years will decrease by 9% while those aged 75 years or more will increase by 110%.16,17
The increase in ACS cases will have a dramatic impact on economic cost. Much of the ACS-associated cost is due to hospital stays, especially in intensive and coronary care units, and to revascularization.12 As official guidelines recommend an early invasive strategy such as angiography plus revascularization for both STEACS and NSTEACS patients,33,34 it is clear that ACS costs will rise accordingly. In addition, the increase in NSTEACS cases will lead to more hospital stays and health care resources use, as this condition causes ischemic recurrences and other complications.34
Although AMI incidence and CAD mortality in Spain are among the lowest in the world, the estimated number of ACS cases is especially high in young men and older women. Efforts to reduce these figures should be implemented through preventive policies. Population-based policies should be designed and applied with a focus on primary prevention and addressed to the whole population, from childhood to old age.35,36 Examples of these policies are the Spanish program NAOS37 (Estrategia para la Nutrición, Actividad Física y Prevención de la Obesidad), or the smoking bans implemented in numerous countries.37 These policies should also be combined with individual interventions in high-risk patients.38,39
Study Characteristics and LimitationsOur estimates of ACS cases are based on the assumption that AMI incidence rates will slightly decrease in the next 8 years and remain stable thereafter, but these assumptions could be conservative. In Spain, AMI incidence rates did not change substantially from 1980 to 2000, as previously reported.5,6 However, it is difficult to compare incidence rates prior to the 2000 AMI definition, which included troponin testing, with more contemporary rates as there is no global consensus on the expected incidence trends. In addition, these trends will probably vary depending on the region and on the population group considered. Using data from the REGICOR study we have observed that AMI crude incidence and hospitalization rates for the whole population did not experience major changes from 2002 to 2008. Nevertheless, there may be differences depending on the sex and age group analyzed.
Two main sources of case-fatality data for AMI were consulted: REGICOR and MASCARA. The MASCARA registry admittedly included nonconsecutive ACS patients, which may have led to low AMI in-hospital case-fatality rates. However, we chose this data source for estimations of 28-day AMI case-fatality because REGICOR covers all consecutive AMI patients. This might lead to varying figures if attempts are made to re-estimate the number of population and of 28-day fatal cases based on the distribution of patients (Table 4) with the rates presented in Table 1.
Our validation analyses reflect a slight overestimation of the number of predicted cases compared to the official statistics, mainly in hospitalized AMI cases. Concerning hospitalized AMI cases, we have to consider that: a) the official morbidity survey is based on a random selection of hospitals and records and some private hospitals do not provide exhaustive data to this survey, and b) this survey does not include AMI cases without complete clinical information or AMI cases within 8 weeks of a previous AMI case. Therefore, we consider that this official survey could underestimate the actual number of ACS events. Thus, our estimates for hospitalized cases would be close to reality in most Spanish autonomous communities. However, we must also consider that hospitalization rates may vary greatly between autonomous communities owing to differences in geographical distribution of population, access to emergency transportation, and access to hospital care. Concerning fatal CAD cases, in our view the small overestimation observed supports the consistency and validity of the main results of this study.
CONCLUSIONSOur results show that ACS cases will increase in Spain in the coming decades. The most significant cause of this increase will be the expansion of the elderly population, which will account for up to 60% of all ACS cases by 2049. The main reduction of 28-day case-fatality has been achieved in hospitalized patients: ACS sudden death remains an unsolved public health problem.
FUNDINGThis study has been funded in part by Instituto de Salud Carlos III- RETIC RD12/0042/0061; RD12/0042/0013-FEDER-ERDF (Red de Investigación Cardiovascular-Programa Heracles), FEDER-FIS (PI081327, PI1101801) and Agència de Gestió d’Ajuts Universitaris i de Recerca-Generalitat de Catalunya (2009 SGR 1195).
CONFLICTS OF INTERESTNone declared.
The authors are grateful to Susanna Tello, Marta Cabañero, Leny Franco, and Isabel Ramió for project and data management. We appreciate the contribution of Anna Puigdefábregas and Rosa Gispert for providing the cross-linkage of our databases with the Mortality Registry from the Catalan Government. We also appreciate the revision of the English text by Elaine Lilly, Ph.D., of Writer's First Aid.