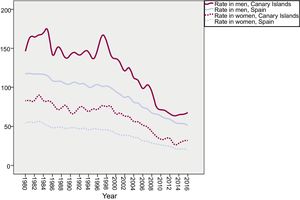
We appreciate the kind interest shown by Martín Cabeza et al. in our article.1 Mortality rates due to cardiac ischemia have exhibited a downward trend during the last 4 decades in the Canary Islands and in Spain as a whole (Figure 1), although the decline in the Canary Islands stopped in 2010.2 Accordingly, the mortality ratio of the Canary Islands to Spain has since increased, reaching almost significant values in 2016: men, 1.33 (95% confidence interval, 0.93-1.93); women, 1.68 (95% confidence interval, 0.96-3.02). This mortality rate is mainly influenced by the living conditions of the population, with the health system a further determinant.

However, the focus of our article was not the mortality of the general population, but that of patients hospitalized for acute myocardial infarction during the years 2007 to 2014. These data represent in-hospital mortality, which is closely related to health care quality. This rate was adjusted for the main risk factors and revealed large inequalities among the different regions. Therefore, we stress that care processes should be reviewed by those responsible for the health system,1 particularly in the communities with the worst results: the Canary Islands, Andalusia, Aragon, the Valencian Community, and Extremadura.
In the Canary Islands, factors that should be analyzed include the time of transfer from regional hospitals (smaller islands of the archipelago) to third-level centers (capital islands) for the performance of primary angioplasty. We agree with our correspondents and have said before that the excess hospital mortality may be related to the late implementation of the Canarian Infarction Code. If so, the coming years should show a marked improvement in the mortality of patients admitted for acute myocardial infarction. Indeed, the implementation of reperfusion networks for acute myocardial infarction has help to reduce mortality in Spain.3