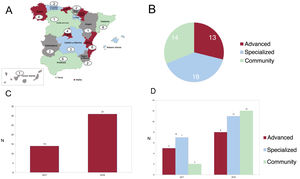


The development of specific heart failure (HF) units has improved the management of patients with this disease due to improved organization and resource management. The Spanish Society of Cardiology (SEC) has defined 3 types of HF units (community, specialized, and advanced) based on their complexity and service portfolio. Our aim was to compare the characteristics, treatment, and outcomes of patients with HF according to the type of unit.
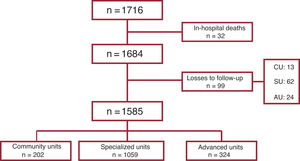
MethodsWe analyzed data from the SEC-Excelente-IC quality accreditation program registry, with 1716 patients consecutively included in two 1-month cutoffs (March and October) from 2019 to 2021 by 45 SEC-accredited HF units. We compared the characteristics, treatment and 1-year outcomes between the 3 types of units.
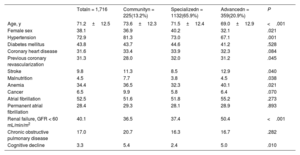
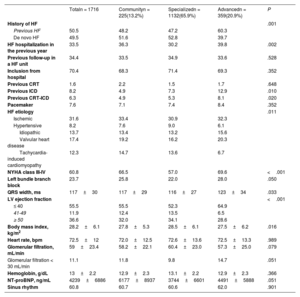
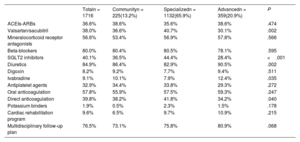
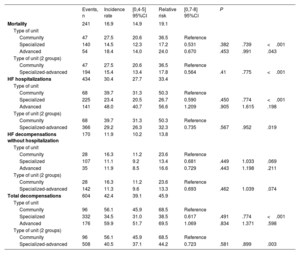
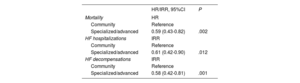
ResultsOf the 1716 patients, 13.2% were treated in community units, 65.9% in specialized units, and 20.9% in advanced units. The rates of mortality (27.5 vs 15.5/100 patients-year; P<.001), admissions for HF (39.7 vs 29.2/100 patients-year; P=.019), total decompensations (56.1 vs 40.5/100 patients-year; P=.003), and combined death/admission for HF (45.2 vs 31.4/100 patients-year; P=.005) were higher in community units than in specialized/advanced units. Follow-up in a community unit was an independent predictor of higher mortality and admissions at 1 year.
ConclusionsCompared with follow-up by more specialized units, follow-up in a community unit was associated with a higher decompensation rate and increased 1-year mortality.
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm