The data of mortality of out-of-hospital sudden cardiovascular death in middle-aged adults have been poorly characterized. The aim of this study is to analyze their epidemiological, clinical and pathological characteristics.
MethodsPopulation observational study of all cardiovascular deaths in people 35–49 years old in Vizcaya between 2003 and 2008. The data of Mortality Register and Forensic Pathology Service were analyzed. The out-of-hospital sudden deaths subjected to forensic autopsy were identified.
Results216 of the 465 cardiovascular deaths were sudden deaths. The main cause was ischemic heart disease (N=140/216). Other conditions were: cardiomyopathies (N=32), cerebrovascular diseases (N=19) and sudden arrhythmic death in structurally normal hearts (N=10). The causes varied significantly in relation to gender and age. Ten percent had been diagnosed in life of a cardiovascular disease; 66% had cardiovascular risk factors and 27% had recently consumed ethanol and/or abuse drugs. The incidence of sudden death was 13.2/100,000 inhabitants/year, representing 46% of cardiovascular deaths. The incidence was 3.77 times higher in males than in females and increased with the age.
ConclusionsThe incidence of sudden death in Vizcaya was lower than in other industrialized countries. In middle-aged adults out-of-hospital sudden cardiac death is the first manifestation of disease in half of all cardiovascular deaths. One challenge in prevention is the development of strategies to identify the highest risk people within the general population at low risk. Studies based on forensic autopsies improve our understanding of cardiovascular mortality.
Keywords
Cardiovascular disease is one of the main causes of mortality in middle-aged adults. A high percentage of these deaths are sudden and affect subjects who have been diagnosed with certain diseases, mainly ischemic cardiopathies.1,2 Various clinical studies have made it possible to determine risk factors for sudden death (SD) in these patients.2,3
In contrast, on other occasions sudden cardiovascular death (SCD) occurs in a non-hospital setting4,5,6,7,8,9,10 and is the first manifestation of disease.2,5,11 The epidemiological, clinical and pathological characteristics of out-of-hospital SD are poorly defined for various reasons: (1) they are not usually included in clinical research studies because they occur unexpectedly in the community; (2) the information sources for most of the available studies are medical death certificates, medical reports, and surveys and interviews of relatives, which leads to a high degree of variability and uncertainty regarding the cause of death12; (3) only a very limited number of studies use data from autopsies to classify the cause of SCD9; (4) the studies based on medical death certificates have limited accuracy6,12 and apparently give considerable overestimations of the incidence of SCD2; (5) papers based on the study of emergency service cases do not usually include cases of unwitnessed out-of-hospital SCD and sometimes have only limited access to medical records2; and (6) differences between studies in the definition of SCD make findings difficult to compare.4,5,6,7,8,9,10
Prospective population studies based on forensic autopsies could provide relevant medical data in the development of prevention strategies for cardiovascular death. Besides making it possible to discover the exact cause of death, this type of study has the advantage of offering histopathological and toxicological data that cannot be determined by other means. In Vizcaya, cases of out-of-hospital SD in young and middle-aged adults are subject to autopsy in the province's only pathology department, which is also in charge of supervising medical death certificates.
This population-based observational study has two main aims:
(1) to analyze the causes of SCD and its clinical and demographic characteristics in subjects of legal medical autopsy, aged 35–49 years; and
(2) to evaluate the incidence of SCD in a well-defined general population and its magnitude in relation to the total number of cardiovascular deaths.
The study was carried out in Vizcaya, an industrial province of the Basque Country with a total population of 1,136,852 inhabitants in 2006; the population between 35 and 49 years of age was 551,636 (280,984 males and 270,652 females).
In accordance with the law, a forensic autopsy (judicial investigation) is necessary in all violent deaths and those where crime is suspected. This includes natural or unexpected sudden deaths in non-hospitalized persons. A medical death certificate, signed by the doctor treating the patient for a previously detected illness, is required in all other natural deaths (without judicial intervention). Via the Basque Institute of Statistics (EUSTAT), the information from the medical death certificates and the forensic autopsy reports reaches the Mortality Register of the Autonomous Community of the Basque Country, where the basic cause of death is selected and codified following the regulations established in the International Classification of Diseases, 10th Revision (ICD-10).13
Data from the Mortality RegisterThe population aged 35–49 who lived in the province of Vizcaya and who died of a disease of the circulatory system (codes I00–I99) or congenital malformations of the circulatory system (codes Q20-Q28) between January 2003 and December 2008 was identified. The following variables were analyzed: sex, age, basic cause of death, place of death (Vizcaya or other provinces) and if the death had been subject to a forensic medical investigation or not.
Data from the Forensic Pathology ServiceSD was defined as that which occurs naturally (non-violent), unexpectedly and within a period of less than an hour from the beginning of the warning symptoms in a person in an apparently good state of health who has not been admitted to hospital and who is performing everyday activities at the time of death. In the unwitnessed deaths or those occurring during sleep, data was included when these people had been seen in a good state of health in the 24h before their death.1,2,7,9
A prospective assessment of the cases was performed. In each case, a complete autopsy was carried out, as well as toxicological and histopathological studies. The medical information and circumstances surrounding the death were also reviewed. This information was obtained from medical reports, police statements and occasionally from interviews with relatives of the deceased. The cause of death was established based on medical and histopathological criteria.
The morphological criteria for the diagnosis of the different causes of SCD have already been published.14,15 In the context of forensic medicine, cardiac arrhythmias correspond to sudden arrhythmic death in structurally normal hearts (SAD), also known as unexplained SD.2,15
Five cardiovascular risk factors (CVRF) were coded: obesity, arterial hypertension, diabetes mellitus, hyperlipidemia and tobacco use. Obesity was defined as having a body mass index ≥30kg/m2 based on autopsy data. Subjects were considered to have suffered hypertension when it appeared on their medical history, if medication for arterial hypertension was found in the chemical–toxicological analysis, or if the histological study detected changes in the small blood vessels of the kidney characteristic of hypertension.16 The deceased was considered to have suffered diabetes mellitus when it appeared on medical records, if the chemical–toxicological analysis revealed hypoglycaemic medication, or if the histopathological study revealed diabetic kidney disease.16 Subjects were considered to have been tobacco users when it appeared on medical records or if the histopathological study detected respiratory bronchiolitis, characteristic finding in smokers.17
Statistical AnalysisThe results are expressed as means (standard deviation) of individual values or as percentages. The Chi-square test was used to assess the possible existence of differences in the distribution of the absolute frequencies in the groups of causes of SCD according to sex and age groups. This test was also used to study the association between the CVRF and the groups of causes of SCD. Only the most common groups (ischemic cardiopathy, myocardial diseases, cerebrovascular diseases and SAD) were included. The Fisher exact test was used to compare qualitative variables with expected counts<5. The significance level chosen was p<.05. All the analyses were performed using the SPSS® program (Statistical Package for Social Sciences).
Epidemiological AnalysisThe resident population of Vizcaya by age and sex was obtained by linear inter- and extrapolation between the censuses in 2001 and 2006 provided by the Basque Institute of Statistics/EUSTAT. The following were calculated for each sex:
– Adjusted rates for age by means of direct standardization with a confidence interval of 95%, using the standard European population as the reference population for the population between 35 and 49 years of age.
– Ratio of standardized rates with a confidence interval of 95% to calculate the relative risk between sexes.
– Specific rates for quinquennial age groups.18
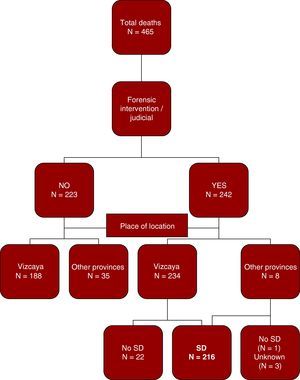
During the six-year study there were 2688 deaths of Vizcaya residents between 35 and 49 years old, 488 from external causes and 2200 from natural causes, of which 346 (16%) were subjected to a forensic autopsy. Deaths due to diseases or congenital malformations of the circulatory system (I00–I99 and Q20–28) totalled 465 (Figure 1). Of the 242 cases involving judicial intervention (medical forensic autopsy), 216 (89%) fulfilled the criteria for SD defined in this study. Besides the 212 cases investigated in the Forensic Pathology Services of Vizcaya, four other cases were identified from the Forensic Pathology Services of other provinces in the Autonomous Community of the Basque Country. The distribution by sex and age of the SCD cases is shown in Table 1.

Figure 1. Diagram showing the distribution of cardiovascular mortality in residents between 35 and 49 years of age. Vizcaya, 2003 and 2008. SD, sudden death.
Table 1. Distribution of the Number of Cases of Sudden Cardiovascular Death with Regard to Sex and Age
| Age groups (years) | Men | Women |
| 35–39 | 28 | 14 |
| 40–44 | 48 | 14 |
| 45–49 | 94 | 18 |
| Total | 170 | 46 |
Ischemic cardiopathy was the most frequent cause of death with 140 cases, including 74 cases of coronary thrombosis and/or acute myocardial infarction and 66 cases with coronary artheromatosis and/or cicatricial myocardial infarction, without thrombosis or acute infarction. After ischemic cardiopathies, the main causes were myocardial diseases (n=32), intracranial hemorrhages and SAD (Table 2).
Table 2. Causes of Sudden Cardiovascular Death (n=216)
| Hypertensive diseases (I10–I15) | |
| Hypertensive cardiopathy | 5 |
| Ischemic heart diseases (I20–I25) | |
| Acute myocardial infarction and/or coronary thrombosis | 74 |
| Chronic ischemic cardiopathy | 66 |
| Cardiopulmonary diseases and pulmonary circulatory disease (I26–I28) | |
| Pulmonary thromboembolism | 4 |
| Other heart diseases (I30–I52) | |
| Dilated myocardiopathy | 14 |
| Left concentric ventricular hypertrophy | 12 |
| Myocarditis | 5 |
| Arrhythmogenic myocardiopathy | 1 |
| Heart arrhythmias (sudden arrhythmic death in a structurally normal heart) | 10 |
| Cerebrovascular diseases (I60–I69) | |
| Intraparenchymal hemorrhage | 11 |
| Subarachnoid hemorrhage | 7 |
| Stroke | 1 |
| Diseases of arteries, arterioles and capillaries (I70–I79) | |
| Dissection of the aorta | 3 |
| Congenital malformations of the circulatory system (Q20–Q28) | |
| Fallot tetralogy | 1 |
| Congenital stenosis of the aortic valve | 1 |
| Anomalous origin of left coronary artery from the pulmonary artery | 1 |
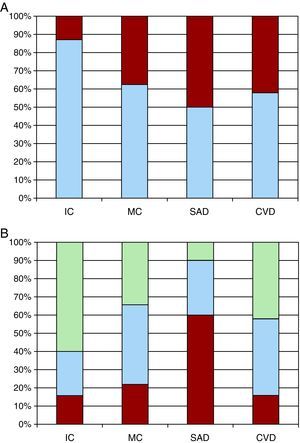
A different distribution of the causes of SCD was observed with regard to sex (p<.001) (Figure 2A). The percentage of males was highest for ischemic cardiopathy (87%) and lowest for SAD (50%). Statistically significant differences were also found with regard to the quinquennial age groups (p=.001): 60% of ischemic cardiopathy cases affected subjects between 45 and 49, while 60% of the SAD cases occurred in people between 35 and 39 (Figure 2B).

Figure 2. Representation of the percentage of cases for each group of causes of sudden death by sex (A) and age groups (B). In A, the blue segment of each bar represents the percentage of men and the red Segment the women. In B, the red segment of each bar represents the percentage of people from 35 to 39 years of age, the blue segment those from 40 to 44, and the green segment those from 45 to 49. CVD, cerebrovascular diseases; IC, ischemic cardiopathy; MD, myocardial diseases; SAD, sudden arrhythmic death in a structurally normal heart.
Clinical Data and Consumption of Toxic Substances in Sudden Death CasesIn 19 of the 183 cases where the medical history was known, heart or cerebrovascular disease had been diagnosed; ischemic cardiopathy was the most common disease (Table 3).
Table 3. Pathological History, Cardiovascular Risk Factors, and Alcohol and Drug Consumption in Sudden Cardiovascular Death
| Cases, n (%) | |
| History of cardiovascular disease in life time | |
| Yes | 19 (9) |
| Ischemic heart disease | 7 |
| Cerebrovascular event | 3 * |
| Hypertensive cardiopathy | 3 |
| Surgery on heart malformations | 3 |
| Dilated myocardiopathy | 2 |
| Mitral-aortic valvulopathy | 1 * |
| Surgery on circle of Willis aneurysm | 1 |
| No | 164 (76) |
| Unknown | 33 (15) |
| Cardiovascular risk factors | |
| None | 74 (34) |
| Tobacco use | 93 (43) |
| Obesity | 53 (24) |
| Arterial hypertension | 46 (21) |
| Hyperlipidemia | 16 (7) |
| Diabetes mellitus | 12 (6) |
| Recent use of alcohol and drugs of abuse | |
| Yes | 58 (27) |
| Alcohol (>0.5g/L in blood) | 27 (12) |
| Cocaine | 18 (8) |
| Cannabis | 17 (8) |
| Opiates | 9 (4) |
| Amphetamines | 4 (2) |
| No | 158 |
* One patient had been diagnosed in lifetime with both diseases.
The most important CVRF was smoking, followed by obesity and arterial hypertension (Table 3). Statistically significant differences were detected in the frequency of smoking (p<.05), arterial hypertension (p<.05) and obesity (p<.01) between the four main groups of causes of SCD. The high frequency of the following risk factors stood out: smoking among the cases of ischemic heart disease (51%); arterial hypertension in cerebrovascular diseases (37%) and obesity in myocardial diseases (53%). The presence of CVRF was particularly low among deaths by SAD (20%).
In the hours prior to death, 27% of the subjects had consumed alcohol or drugs of abuse, cocaine being the most frequent (Table 3).
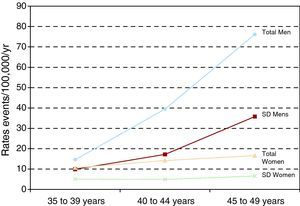
Rates of Mortality from Sudden Death and in the Total Number of Cardiovascular DeathsThe standardized rate of SCD was 13.20 (CI 95% 11.44–14.97) per 100,000 inhabitants, 21.0 (IC 95% 11.44–14.97) in men and 5.57 (IC 95% 3.96–7.18) in women. The relative risk of SCD was significantly higher in males than in females (standardized rate ratio=3.77; CI 95% 2.78–5.11). Variations were observed for the quinquennial age groups in the specific rate of SCD: 7.57 per 100,000 inhabitants for subjects between 35 and 39 years of age; 11.07 for 40–44-year-old subjects and 20.98 for those between 45 and 49. The progressive increase in the rates with age was almost exclusively a consequence of an increase in male cases (Figure 3).

Figure 3. Specific mortality rates per 100,000 people per year for the total of cardiovascular deaths and for sudden cardiovascular death in people from 35 to 49 years of age by sex and quinquennial age groups. Vizcaya, 2003 and 2008. SD, sudden death.
SCD represented 46% of the total number of cardiovascular deaths. With regard to the diagnostic groups, the highest percentage of SD was observed in deaths due to arrhythmias, myocardial diseases and ischemic heart disease; cerebrovascular diseases stood out for being quite the opposite, with a low percentage of SD (Table 4).
Table 4. Comparison of the Rates of Sudden Cardiovascular Death (SCD) with the Mortality Rates of the Total Number of Cardiovascular Deaths (TCD) in People Between 35 and 49 Years of Age by Groups of Diseases in the International Classification of Diseases 10th Revision
| SCD | TCD | SCD/TCD x 100 | |
| Chronic rheumatic heart diseases (I05–I09) | 0 | 0.2 | 0 |
| Hypertensive diseases (I10–I15) | 0.3 | 0.6 | 50 |
| Ischemic heart diseases (I20–I25) | 8.5 | 13.7 | 62 |
| Cardiopulmonary diseases and pulmonary circulatory disease (I26–I28) | 0.2 | 0.4 | 50 |
| Other heart diseases (I30–I52) | |||
| Myocardial diseases | 1.9 | 2.9 | 65 |
| Heart arrhythmias (sudden arrhythmic death in a structurally normal heart) | 0.6 | 0.9 | 66 |
| Remainder | 0 | 1.5 | 0 |
| Cerebrovascular diseases (I60–I69) | 1.1 | 6.4 | 17 |
| Diseases of arteries, arterioles and capillaries (I70–I79) | 0 | 0.1 | 0 |
| Congenital malformations of the circulatory system (Q20–Q28) | 0.2 | 0.5 | 40 |
The highest percentage of SD of all the cardiovascular deaths was among subjects between 35 and 39 years of age (60% vs. 41% for ages 40–44 and 45% for ages 45–49).
DiscussionAccording to our study, approximately half the cardiovascular deaths in adults between 35 and 49 years of age are SCD investigated by the forensic pathology services. In most cases there is no history of heart and/or cerebrovascular disease in their lifetime, these deaths occurring totally unexpectedly and unpredictably in the community. On the other hand, the frequency of CVRF is high and a substantial percentage of subjects had previously consumed alcohol and/or drugs of abuse. These data have important clinical implications with regard to possible prevention strategies for SCD in the general population.
Epidemiological DataThe incidence of SCD in Vizcaya was 13.2 cases per 100,000 inhabitants per year. This rate is lower than that observed in studies in North America and northern Europe (with a study population of ages similar to this study), in which the incidence ranges from 20 to 40 cases per 100,000 inhabitants per year.7,9 Other studies of out-of-hospital SCD in the south of Europe have also described lower mortality rates than in other industrialized countries.4,10
The risk of SCD was nearly 4 times higher in men than in women, which is similar to results described in the province of Girona,4 and somewhat more pronounced than the difference observed in other studies, in which the incidence in men doubled or tripled that of women.6,8,9
In accordance with previous population-based studies, we observed that the incidence of SCD increases progressively with age.4,6,7,8,9 The rate in subjects between 45 and 49 years of age nearly tripled that of subjects between 35 and 39, and is close to that observed in the Girona study4 in people ages 45–54 (28 cases per 100,000 inhabitants per year). It is significant that this increase was almost exclusively due to the increase in the rates in men; the incidence in women remained very stable.
Causes of Sudden DeathIschemic cardiopathies were the main cause, with 65% of the total number of SCD, a similar figure to that observed in other studies.7,9,19 Regarding the mechanisms responsible for the SD, and in accordance with the results of previous studies,20 half of the SD of ischemic origin are due to a new acute ischemic event, while the other half are secondary to ventricular arrhythmias triggered in a ventricle with old infarct-related lesions, but without acute coronary lesions. After ischemic cardiopathies, myocardial diseases are the largest group, with a frequency ranging between 10% and 15%.2,9 Intraparenchymal and subarachnoid brain hemorrhages are also known causes of SD. Finally, it is necessary to highlight SAD or unexplained SD.2,15,21 Nowadays, it is thought that many of these cases are inherited arrhythmias, where alterations are located in the ion channels (channelopathies). The most important are long QT syndrome, Brugada syndrome, short QT syndrome and catecholaminergic polymorphic ventricular tachycardia. In recent years, thanks to advances in genetic research, mutations in genes that code ion channels have been found in cases that had initially been classified as unexplained SD21. For this reason, it is essential that molecular biology studies be included in the near future in the post-mortem investigation protocol for SAD (molecular autopsies).22
Another important finding was that the distribution of the causes of SCD varied significantly with regard to the demographic variables. With regard to sex, it was noteworthy that 87% of the deaths from ischemic cardiopathies were men. However, the percentage of women in the other groups was higher, and it stands out that 50% of the SAD cases were female. The percentage of ischemic cardiopathies increases progressively with age,9 and in this series it was particularly high among people between 45 and 49 years of age. In contrast, SAD is more common in younger adults.2,15
The epidemiological and etiological characteristics of SCD in children and young adults are very different from those of middle-aged adults. In a previous study of SD in Vizcaya in people from 1 to 35 years of age, we found that the incidence of SCD was 9 times lower than in this study, and that SCD was due to a wide variety of causes, with none reaching a clear statistical predominance.23
Clinical Data and Prevention of Sudden DeathIn developed countries, SCD is responsible for nearly half of cardiovascular deaths and it is the first manifestation of disease in 20%–40% of these cases.5,11,19,24 The morphological substrate is frequently asymptomatic or is not detected. In our series, SD was the first known manifestation of the disease in 40% of all the cardiovascular deaths (sudden or not) and only 10% of the SCD victims had previously been diagnosed with a cardiac or cerebrovascular disease.
Due to the high percentage of subjects with no previously known disease, early identification of subjects with a high risk of SCD in the community is not possible, making primary prevention extremely difficult. One of the basic challenges lies in identifying high risk subjects within the low risk population.
The prevalence of CVRF is very high in SCD.1,19,24 Asymptomatic individuals with CVRF have a risk of SD that is lower than those with manifestations of the disease, but higher than the general population. One possible way of reducing the incidence of SCD in the community is identifying and treating CVRF.
Smoking, morbid obesity and arterial hypertension have been considered independent CVRF for SD.1,2,19 There was a high frequency of these CVRF in the Vizcaya sample, with the different distributions with regard to the morphological substrate of the SCD being noteworthy. Significantly higher frequencies were found of tobacco use in ischemic cardiopathy, of hypertension in brain hemorrhages, and of obesity in cases of myocardiopathy. In contrast to the rest of the causes, the low frequency of CVRF in SAD stood out.
The consumption of certain illicit drugs (mainly cocaine) and ethyl alcohol can precipitate SD through diverse mechanisms in a predisposed individual.1,2 The frequency of recent consumption of these substances was relatively high (27%), suggesting another possibility for preventing these deaths by reduction of factors which can trigger SD.
On the other hand, our data also show the importance of improving out-of-hospital cardiopulmonary resuscitation systems to improve the survival rates of these patients.
Some SCD are due to genetic heart disorders (myocardiopathies and channelopathies), which are usually inherited with a dominant autosomal pattern. As SD is often the first manifestation of the disease, forensic pathology plays an important role in the development of strategies aimed at identifying asymptomatic relatives and preventing possible future deaths in the same family.
LimitationsThe comparison of data from out out-of-hospital SCD series has important limitations due to the differences in methodologies: (1) in the chronological criteria for the definition of SD; (2) in the sources used for obtaining data; and (3) in the inclusion and exclusion criteria. In this series, only those cases subjected to a legal medical autopsy because of the unexpected nature of the death were included as SCD. Some of the deaths for which a medical death certificate was issued could have been out-of-hospital SCD in patients who had previously been diagnosed with a disease, so it is possible that our study has underestimated the incidence compared with other studies which included these cases. Assuming this limitation, the incidence of SCD in our study seems to be in agreement with the pattern of cardiovascular mortality in Europe, where the Basque Country has the lowest rates of cardiovascular mortality25 and also with the incidence found in other studies of southern Europe, which reveal lower rates than other industrialized countries.4,10 Although the reasons are not well known, there seem to be many: the prevalence of CVRF; lifestyle habits, diet and physical activity; access to medical services; and genetic and environmental factors.25
The correlation between autopsy findings and the cause of death should be interpreted with care. In certain pathologies, the degree of certainty is not in question (e.g. coronary thromboses or intracranial hemorrhages), while in others the diagnosis is only probable and based on exclusion (e.g. chronic ischemic cardiopathies or myocardiopathies).
ConclusionsHalf of the cardiovascular deaths in people aged 35–49 are out-of-hospital SCD investigated by the forensic services. The incidence of SCD in Vizcaya was 13.2 cases per 100,000 inhabitants per year, lower than that found in other industrialized countries. The rate among men is almost 4 times higher than that among women, and increased progressively with age. Ischemic cardiopathies were the most common cause of SCD, followed by myocardiopathies, brain hemorrhages and primary arrhythmias. The distribution of the causes of death differs greatly with regard to sex and age. The prevention of SCD is made much more difficult by the fact that it is impossible to identify high-risk subjects, since SD is commonly the first manifestation of the disease. The frequency of CVRF and the recent consumption of alcohol and/or drugs of abuse are relatively high, so detection and control strategies for these factors could be effective in the prevention of SCD.
Molecular biology analyses are necessary: (1) because they may be the only tool in SAD which makes it possible to discover gene mutations associated with channelopathies and thus discover the cause of death; and (2) in family prevention strategies. Pathology and molecular biology services should collaborate in carrying out genetic studies. Until that happens, it would be a good idea for pathology services to store a suitable number of samples (frozen blood and myocardium).
The findings of this study underline the need to improve the investigation of out-of-hospital SCD in the community, a field about which there are few studies in the medical literature. Research based on forensic autopsies provides useful and reliable epidemiological and clincopathological information about cardiovascular mortality.
Conflicts of interestThe authors state that they have no conflicts of interest.
Received 21 April 2010
Accepted 20 July 2010
Corresponding author: Servicio de Patología Forense de Vizcaya, Instituto Vasco de Medicina Legal, Barroeta Aldamar 10, planta -1, 48001 Bilbao, Vizcaya, Spain. morentin.b@aju.ej-gv.es