Obesity is a major cardiovascular risk factor. In Spain, few studies have physically measured height and weight to estimate the magnitude of the problem. The aim of this study was to determine the prevalence of child and adolescent obesity in Spain in 2012.
MethodsWe performed a cross-sectional probability sample of 1018 children, representative of the Spanish population aged between 8 and 17 years old, with objectively measured height and weight, along with other sociodemographic variables. We calculated the prevalence of overweight and obesity according to the criteria of the World Health Organization, the International Obesity Task Force, and the enKid study.
ResultsIn the group aged 8 to 17 years old, the prevalence of overweight and obesity was 26% and 12.6%, respectively; 4 in 10 young people were overweight or obese. Excess weight was found in 45% of the group aged 8 to 13 years and in 25.5% of that aged 14 to 17 years. This cardiovascular risk factor was associated with lower social class and lower educational level.
ConclusionsThe prevalence of overweight and obesity in children and adolescents in Spain remains high (close to 40%), but has not increased in the last 12 years.
Keywords
.
INTRODUCTIONCardiovascular disease is a leading cause of mortality and hospitalization in Spain and is a major contributor to health costs. Each year, this entity causes approximately 120 000 deaths and led to 5 million hospital stays in 2006 alone.1–3 At present, the fight against cardiovascular disease focuses particularly on the development of secondary and tertiary prevention measures. However, to date, efforts to address modifiable risk factors present in individuals over a long period, sometimes since childhood (e.g., obesity) have not been a priority.
Obesity is an enormous medical and public health issue.4 Numerous studies have shown a strong relationship between obesity and cardiovascular disease.5–13
The association between obesity and cardiovascular disease concerns both adult obesity and obesity at earlier ages.13,14 In childhood and adolescence, excess weight is directly associated with elevated plasma insulin, lipid and lipoprotein concentrations, and hypertension15 and can cause the premature onset of cardiovascular disease in adults.16–20
The worldwide rise in overweight and obesity in childhood and adolescence in recent years has been dramatic.2,3 It is estimated that around one third of all children are overweight.21 In Spain, the prevalence of child obesity is among the highest in Europe, together with Malta, Italy, Greece, and the United Kingdom.22–24 In 2010 the SESPAS (Spanish Society of Public Health and Health Administration) reported that 35% of children had excess weight (20% were overweight and 15% were obese), making this phenomenon an increasingly important and highly significant risk factor, whose trend should be rigorously and systematically monitored. Methodological weaknesses related to the definition and measurement of obesity and sample selection are, however, common.
Consensus is lacking on the criterion that should be used to establish overweight or obesity using body mass index (BMI). The 2 criteria most widely accepted by the international community are those proposed by the World Health Organization (WHO)26 (overweight: specific BMI values according to age and sex, >+1 standard deviation in the reference population defined by the WHO25; obesity: sex- and age-specific BMI values, >+2 standard deviations) and those proposed by the International Obesity Task Force (IOTF)26 (cutoff points for childhood overweight or obesity specific to each BMI value and sex, using the reference population specified by the IOTF26). In Spain, tables published by the Fundació F. Orbegozo are also widely employed.27,28 These tables were used in the enKid study29,30 (evaluating dietary habits and nutritional status of children and young people in Spain [1998-2000]), a national benchmark study on child obesity, dietary habits, and lifestyle in children and adolescents, whose age- and sex-specific cutoff points were the 85th percentile for overweight and the 95th percentile for obesity. In addition to the lack of a consensus definition of obesity, hindering comparisons among studies, the available data are often drawn from investigations (mainly health surveys) that did not measure height and weight directly, but were based on estimations reported by the participants or their parents or guardians, leading to a bias that usually underestimates the prevalence of obesity.31–37 In Spain, the 2 most recent national studies used direct height and weight measurement: the enKid study, performed between 1998 and 2000 in the population aged 2 to 24 years and the recent ALADINO (ALimentación, Actividad física, Desarrollo INfantil y Obesidad [in English, Diet, Physical Activity, Childhood Development and Obesity] study,38 which conducted fieldwork between October 2010 and May 2011 among boys and girls aged 6 to 9.9 years old.
The present investigation was designed independently from the enKid and ALADINO studies for the purpose of determining the prevalence of child and youth overweight and obesity in 2012 in Spain using direct and standardized weight and height measurements, based on the main definitions of child obesity currently in effect.
METHODSWe conducted a cross-sectional, observational study in a population-based probability sample in which the study population was composed of children and adolescents of both sexes aged 8 to 17 years old residing in family homes in mainland Spain. All fieldwork was carried out between 10 April and 31 May, 2012.
A complex probabilities sample was used, in which the sample was stratified by multistage conglomerates with selection of the primary sampling units (municipality) and secondary units (census sections) with probability proportional to size sampling, and tertiary units (homes) and final units (individuals), by a combined system of random routes-itineraries and sex and age quotas. Population strata were formed by crossing 15 autonomous communities in mainland Spain with municipality size, divided into 5 categories: ≤2000; 2001-10 000; 10 001-50 000; 50 001-200 000, and >200 000 inhabitants. The sample was fixed proportionally to stratum size; thus, the study sample and population showed equal distributions in both age brackets of the minors studied (8-13 and 14-17 years).
Height and weight were measured in the presence of the adult responsible for the study subject's diet (usually the mother, father, or guardian), who also answered the sociodemographic questions (Computer Assisted Personal Interview). A weighing scale and height tape measure were used to collect the anthropometric measurements of the various members of the household, following a specific measurement protocol. The specific models used were: a) Tefal® PP1027 A9 scale, and b) Soehnle® 5002.01.001 wall-mounted tape measure. BMI was determined by applying the formula obtained when dividing the weight (kilograms) by the square of the height (meters).
The variables initially included in the study had the following levels: a) the subject's age bracket (8-13 years, 14-17 years); b) the subject's sex; c) municipality size (≤2000; 2001-10 000, 10 001-50 000, 50 001-200 000, and >200 000 inhabitants); d) educational level of the person responsible for the child's diet (specifying all completed years for primary education, compulsory secondary education, and high school, vocational training, university degrees, and postgraduate work); e) employment status of the person responsible for the subject's diet (working, unemployed but previously worked, seeking first employment, retired [previously worked], homemaker, student, disabled, permanent disability, others), and f) occupation of father, mother, or guardian (highest according to the National Occupational Classification 2011). Some variables were subsequently recoded, as shown in the table, due to the low number of observations or because these variables behaved similarly to the dependent variable.
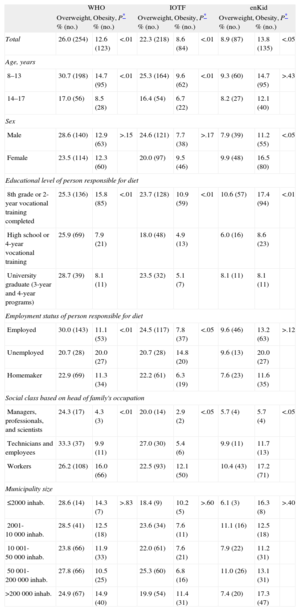
Prevalence of Overweight and Obesity in the Child and Youth Populations in Spain According to the World Health Organization, International Obesity Task Force, and EnKid Criteria, 2012
| WHO | IOTF | enKid | |||||||
| Overweight, % (no.) | Obesity, % (no.) | P* | Overweight, % (no.) | Obesity, % (no.) | P* | Overweight, % (no.) | Obesity, % (no.) | P* | |
| Total | 26.0 (254) | 12.6 (123) | <.01 | 22.3 (218) | 8.6 (84) | <.01 | 8.9 (87) | 13.8 (135) | <.05 |
| Age, years | |||||||||
| 8–13 | 30.7 (198) | 14.7 (95) | <.01 | 25.3 (164) | 9.6 (62) | <.01 | 9.3 (60) | 14.7 (95) | >.43 |
| 14–17 | 17.0 (56) | 8.5 (28) | 16.4 (54) | 6.7 (22) | 8.2 (27) | 12.1 (40) | |||
| Sex | |||||||||
| Male | 28.6 (140) | 12.9 (63) | >.15 | 24.6 (121) | 7.7 (38) | >.17 | 7.9 (39) | 11.2 (55) | <.05 |
| Female | 23.5 (114) | 12.3 (60) | 20.0 (97) | 9.5 (46) | 9.9 (48) | 16.5 (80) | |||
| Educational level of person responsible for diet | |||||||||
| 8th grade or 2-year vocational training completed | 25.3 (136) | 15.8 (85) | <.01 | 23.7 (128) | 10.9 (59) | <.01 | 10.6 (57) | 17.4 (94) | <.01 |
| High school or 4-year vocational training | 25.9 (69) | 7.9 (21) | 18.0 (48) | 4.9 (13) | 6.0 (16) | 8.6 (23) | |||
| University graduate (3-year and 4-year programs) | 28.7 (39) | 8.1 (11) | 23.5 (32) | 5.1 (7) | 8.1 (11) | 8.1 (11) | |||
| Employment status of person responsible for diet | |||||||||
| Employed | 30.0 (143) | 11.1 (53) | <.01 | 24.5 (117) | 7.8 (37) | <.05 | 9.6 (46) | 13.2 (63) | >.12 |
| Unemployed | 20.7 (28) | 20.0 (27) | 20.7 (28) | 14.8 (20) | 9.6 (13) | 20.0 (27) | |||
| Homemaker | 22.9 (69) | 11.3 (34) | 22.2 (61) | 6.3 (19) | 7.6 (23) | 11.6 (35) | |||
| Social class based on head of family's occupation | |||||||||
| Managers, professionals, and scientists | 24.3 (17) | 4.3 (3) | <.01 | 20.0 (14) | 2.9 (2) | <.05 | 5.7 (4) | 5.7 (4) | <.05 |
| Technicians and employees | 33.3 (37) | 9.9 (11) | 27.0 (30) | 5.4 (6) | 9.9 (11) | 11.7 (13) | |||
| Workers | 26.2 (108) | 16.0 (66) | 22.5 (93) | 12.1 (50) | 10.4 (43) | 17.2 (71) | |||
| Municipality size | |||||||||
| ≤2000 inhab. | 28.6 (14) | 14.3 (7) | >.83 | 18.4 (9) | 10.2 (5) | >.60 | 6.1 (3) | 16.3 (8) | >.40 |
| 2001-10 000 inhab. | 28.5 (41) | 12.5 (18) | 23.6 (34) | 7.6 (11) | 11.1 (16) | 12.5 (18) | |||
| 10 001-50 000 inhab. | 23.8 (66) | 11.9 (33) | 22.0 (61) | 7.6 (21) | 7.9 (22) | 11.2 (31) | |||
| 50 001-200 000 inhab. | 27.8 (66) | 10.5 (25) | 25.3 (60) | 6.8 (16) | 11.0 (26) | 13.1 (31) | |||
| >200 000 inhab. | 24.9 (67) | 14.9 (40) | 19.9 (54) | 11.4 (31) | 7.4 (20) | 17.3 (47) | |||
Inhab., inhabitants; IOTF, International Obesity Task Force; WHO, World Health Organization.
The prevalences of overweight and obesity with their respective 95% confidence intervals (95%CI) were calculated for general data. All confidence intervals were calculated using bootstrap techniques,39 based on 1000 samples, and the proportions were compared using the chi-square statistic when the conditions for the test were met, or the Fisher exact test if otherwise. SPSS version 18 was used for the statistical analyses.
RESULTSAmong the individuals in the study population contacted, a collaboration rate (individuals who completed the questionnaire and underwent the respective measurements) of 80% was achieved. The final sample consisted of 978 subjects.
The Table contains estimates of the prevalences of overweight and obesity in children and adolescents of both sexes according to the WHO, IOTF, and enKid study criteria, based on the Fundación F. Orbegozo tables for the entire study population as a function of the sociodemographic variables considered. This table shows that the obesity data pattern that appears with the IOTF criteria is very similar to that found using the WHO criteria, although the percentages were systematically lower than those provided by the WHO. When the WHO or IOTF criteria were applied, the prevalences of overweight tended to be 2- or 3-fold, or sometimes even 4-fold, the prevalences of obesity; this was true for all the sociodemographic variables studied. However, when the enKid criteria were applied, the data pattern was inverted and the prevalences of overweight tended to be similar to or even lower than those of obesity.
When the WHO criteria were used, the prevalence of overweight was 26.0% (95%CI, 23.2%-28.8%) for the Spanish population aged 8–17 years; the prevalence of obesity was 12.6% (95%CI, 10.7%-14.8%), and total excess weight (overweight plus obesity) was 38.6% (95%CI, 35.5%-41.6%). Problems with obesity were more common in the group aged 8-13 years than in those aged 14-17: 30.7% were overweight and 14.7% were obese in the first group compared to 17.0% and 8.5%, respectively, in the second group (P<.01).
By sex, 28.6% of Spanish boys were overweight and 12.9% were obese compared with 23.5% and 12.3% of Spanish girls, respectively. No statistically significant differences were observed between childhood and adolescent overweight and obesity in either sex according to municipality size. The educational level of the person responsible for the child's diet (mother in 85% of subjects; father in 14%) was statistically associated with the prevalence of obesity or overweight. In particular, the highest percentage of child obesity was seen when the person responsible for the children's diet and care had only finished 8th grade or the first 2 years of vocational training.
The prevalence of obesity was significantly higher in the lower social classes and in children whose parents were unemployed, a common observation regardless of the criteria used to define weight problems.
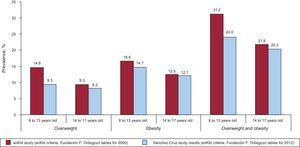
The Figure illustrates the trend in the overweight and obesity prevalences in children and adolescents between 2000 and 2012 in Spain. The results of the enKid study (1998-2000) and our 2012 data are compared by using the criteria applied by the enKid study based on the Fundación F. Orbegozo reference tables. Both age brackets (8-13 and 14-17 years) showed similar prevalences of obesity and overweight, but with a slightly downward trend in 2012.
DISCUSSION
A total of 38.6% of Spanish children and adolescents of both sexes aged between 8 and 17 years have excess weight according to the WHO criteria. Consequently, approximately 4 in 10 Spanish young people are exposed from very early stages to potentially modifable cardiovascular risk factors and to short- and long-term health effects. This problem is accentuated in subjects who were younger and in lower socioeconomic levels, contributing to increases in current and future health inequalities.
Recent studies have shown notable differences in obesity and overweight among various European countries.40,41 In a cross-sectional study published in 2011 on height and weight measurements in children aged 10 to 12 years from 7 European countries,42 the differences in excess weight (overweight plus obesity) ranged from 44.4% of boys in Greece to 13.5% of girls in Belgium. The figures in Spain are high; indeed, they are among the highest in Europe and are similar to those of the United States (the paradigm of the worldwide obesity pandemic) where the prevalence of excess weight is 37.1% in children aged 6-11 years and 34% in adolescents aged 12-19 years.43,44
The SESPAS 2010 reports that 35% are overweight which, compared with our data, would indicate a slightly upward trend. When analyzing trends in problems with overweight among the child population in Spain and other countries, common difficulties are encountered in the definition and measurement of obesity used in each study. Only a few studies have employed direct physical measurement of weight and height among children and adolescents in Spain, and studies based on parents’ perception of their children's height and weight (most studies) usually underestimate BMI, as it is common to underestimate weight and overestimate height. In Spain, both the enKid study, which was carried out between 1998 and 2000, and the ALADINO study, conducted between October 2010 and May 2011, worked with direct measurements. Serial studies such as these will provide information on trends in the prevalence of child obesity among the Spanish population over time. However, the characteristics of the study populations and the criteria for overweight and obesity used in these studies hamper comparisons.
When we applied the enKid criteria to our 2012 data and compared the current prevalences of obesity with those of the 2000 enKid study (in both cases, taking the reference population in the Fundación Orbegozo tables as our own reference), levels of overweight and obesity have apparently held steady or dropped slightly. If this is a true reflection of reality, an important finding was that estimates obtained by using the enKid criteria and by applying the Fundación F. Orbegozo tables to our data (overweight, 22.7%) are much lower than those obtained with the IOTF (30.9%) or WHO (38.6%) criteria and the respective reference populations for the age bracket of 8-17 years.
In terms of the sociodemographic variables used to disaggregate the prevalences, in most countries belonging to the OECD (Organization for Economic Co-operation and Development), boys show higher percentages of overweight and obesity than girls (except in Scandinavian countries, such as Sweden, Norway, and Denmark). Likewise, obesity predominates, as our data indicate, among those who are poor and have a lower educational level.45–48
Despite the efforts of health authorities and professionals to monitor and reduce the high prevalences of overweight at all ages, in particular among children and youth (due to the impact in adulthood and the potential to develop prevention habits), the data seem to indicate that efforts are failing. The recent 2012 OECD report44 appears to support this conclusion. Because of the association between cardiovascular risk factors in general (particularly obesity) and cardiovascular disease as the leading cause of death in industrialized nations, it is imperative to take further measures to design and implement public health policies that reduce this dramatic problem, in order to save thousands of human lives each year, to improve public health and well-being, and to lessen the financial burden on society. Regular, standardized, and methodologically adequate studies are needed to accurately monitor the extent and trend of childhood and adolescent obesity, which is an avoidable and modifiable problem, given that the cause is usually exogenous due to a caloric imbalance related to diet and inadequate physical activity.
LimitationsOne of the limitations of this study is that, although BMI is a widely accepted and extensively used indicator in epidemiologic studies on the prevalence of obesity, it is an indirect indicator that usually underestimates actual levels of obesity, particularly in childhood and adolescence.49 In addition, there is debate on which criteria should be used in BMI-based definitions of childhood and youth obesity and overweight and on which reference population is the most appropriate. In this study, we used the 2 criteria and reference populations that are most widely accepted by the international community (WHO and IOTF) and other criteria that are widely used in the Spanish setting (the enKid criteria applied to Fundación F. Orbegozo reference tables).
CONCLUSIONSThe prevalence of overweight and obesity in the Spanish population aged 8-17 years in 2012 is 26.0% and 12.6%, respectively, indicating that approximately 4 in 10 Spanish young people in these age brackets have the cardiovascular risk factor of excess weight.
The prevalence of excess weight is slightly higher in boys than in girls, and is much higher in the age bracket of 8-13 years. This risk factor is associated with lower social classes or educational levels, regardless of the criteria used to define obesity.
Despite the methodological limitations of this study, the extent of this problem in Spain appears to have stabilized over the past decade, although levels remain too high.
FUNDINGMinisterio de Economía y Competitividad del Reino de España (Acción Estratégica en Salud), Instituto de Salud Carlos III-FEDER. File PI10/02018.
CONFLICTS OF INTERESTNone declared.