The aim of this study was to compare the prevalences of obesity, diabetes and other cardiovascular risk factors in the region of Andalusia with those in the rest of Spain.
MethodsThe Di@bet.es study is a national, cross-sectional, population-based survey of cardiometabolic risk factors and their association with lifestyle. The sample consisted of 5103 participants ≥ 18 years. The variables analyzed were clinical, demographic and lifestyle survey, physical examination, and oral glucose tolerance test. The prevalence of cardiovascular risk factors in Andalusia (n=1517) was compared with that for the rest of Spain (n=3586).
ResultsIn data adjusted to the Spanish population, the prevalence of diabetes (World Health Organization, 1999), hypertension (blood pressure ≥ 140/90mmHg), high-sensitivity CRP levels (≥ 3mg/L) and obesity (body mass index ≥ 30kg/m2) were 16.3%, 43.9%, 32.0%, and 37.0% in Andalusia compared with 12.5%, 39.9%, 28.3%, and 26.6% in the rest of Spain (P<.001 for differences except P=.01 for the difference in high-sensitivity CRP levels). The corresponding figures for the Andalusia data adjusted to the Andalusian population were 15.3%, 42.3%, 31.4%, and 34.0%, respectively. Differences in diabetes, hypertension and high-sensitivity CRP were not significant in models adjusted for age, sex, and adiposity measurements. Differences in obesity were not significant in models adjusted for age, sex, educational level, marital status, work status, and physical activity (P=.086)
ConclusionsThis study contributes information from a national study perspective and shows a higher prevalence of cardiovascular risk factors in southern Spain, in close relation to obesity, a sedentary lifestyle, and markers of socioeconomic disadvantage.
Keywords
Cardiovascular disease (CVD) is one of the leading causes of death, morbidity and health expenditure in industrialized countries, as well as in many developing areas.1 As in other societies, CVD is the primary cause of death in the Spanish population, accounting for 32% of all deaths.2 The detection and control of cardiovascular risk factors (CVRF) remains the essential preventive strategy.3 In this regard, smoking,4 hypertension,5 hypercholesterolemia,6 and diabetes mellitus7 (DM) are classical, well-established modifiable CVRF. Obesity is a central contributor, both as an independent risk factor for CVD 8 and also through its association with a high burden of other CVRF, including hypertension,9 dyslipidemia,10 and type 2 DM,11 as well as many other conditions. More recently, high levels of high-sensitivity C-reactive protein (CRP), a sensitive marker of low-grade systemic inflammation linked to obesity and features of the metabolic syndrome, have also emerged as a novel candidate for the prediction of CVD events.12
Prevalence studies of CVRF are of great interest to define health policies for cardiovascular prevention. Possible regional differences in such prevalence rates are also important because they may be used for resource allocation and to infer the success or otherwise of area-based policies to tackle CVD.
The Di@bet.es study is a national cross-sectional, epidemiological study, designed to examine the prevalence of obesity, DM, and other CVRF in Spain13. The sample corresponding to Andalusia (an autonomous region in southern Spain) was enlarged to include specific regional data. These data are of great interest as recent reports on the incidence of CVD in Spain show that Andalusia is the Spanish region with the highest rates of CVD mortality, although the reasons for this are not clearly established.2 The aim of this study was to compare, from a national study perspective, the prevalence of obesity, DM, and other CVRF in the region of Andalusia with those in the rest of Spain.
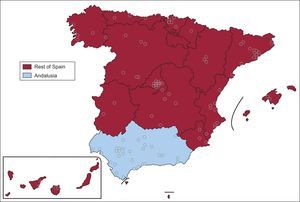
METHODSThe Di@bet.es study is a national, cross-sectional, population-based survey conducted in 2009 to 2010.13 A cluster sampling design was used to select participants to form a representative random sample of the Spanish population, using the Spanish health system register that covers more than 99% of the Spanish population. In the first stage, 100 health centers or their equivalent were selected from all around the country, with a probability proportional to their population size, after which 100 individuals ≥ 18 years were randomly selected from each health center. The sample corresponding to Andalusia was enlarged to provide representative population-based data. The minimum sample size needed for these regional estimations was set on 784 and 1291 for estimations on the prevalence of DM and obesity respectively (precision level, 2.5%; confidence interval 95% [CI95%]; expected prevalence of diabetes, 15%; expected prevalence of obesity, 30%) The extension involved increasing the number of health centers selected from Andalusia from the original 18 to 30 and also an increase in the number of individuals selected from each center from 100 to 120. The Figure shows a detail of the 112 clusters that were finally included in the Di@bet.es study (30 clusters from Andalusia, 82 clusters from the rest of Spain).
 selected in the Di@bet.es study.")
The study was approved by the Ethics and Clinical Investigation Committee of Carlos Haya Hospital (Malaga, Spain) in addition to other regional ethics and clinical investigation committees all over Spain, and written informed consent was obtained from all the participants.
Variables and ProceduresThe participants were invited to attend a single examination visit at their health center. Information was collected using an interviewer-administered structured questionnaire, followed by a physical examination. Fieldwork was undertaken by 7 teams, each comprising a nurse and dietitian who, prior to the study, had undergone a specific training course to standardize procedures. After the interview, fasting blood sampling and an oral glucose tolerance test were performed.
Information on age, sex, educational level, marital status, work status, and smoking habits was recorded. Food consumption was determined by a 40-item food frequency questionnaire14 and adherence to a Mediterranean diet was estimated by a previously validated 14 item score.15 The level of daily physical activity was estimated by the short form of the International Physical Activity Questionnaire.16,17 Weight, height, and waist and hip circumferences were measured by standardized methods. The body mass index was calculated. Blood pressure was measured using a blood pressure monitor (Hem-703C, Omron, Barcelona, Spain) after several minutes in a seated position; the mean of 2 measurements taken 1 to 2min apart was used for analysis. Participants with baseline capillary blood glucose levels lower than 7.8 mmol/L and not receiving treatment for DM underwent a standard oral glucose tolerance test, obtaining fasting and 2-h venous samples. Samples were immediately centrifuged and serum was frozen until analysis. Serum glucose, triglycerides and cholesterol were measured enzymatically, and high-density lipoprotein cholesterol by a direct method. Low-density lipoprotein cholesterol was estimated by the Friedewald formula.
Definition of Cardiovascular Disease Risk FactorsThe diagnosis of DM was based on the 1999 World Health Organization criteria.18 Not all the participants agreed to undergo the oral glucose tolerance test and therefore the prevalence of unknown DM was calculated as: (number of diagnosed oral glucose tolerance test cases/number of participants who underwent the oral glucose tolerance test) ×(1−known DM prevalence). The total prevalence of DM was then calculated as known DM + unknown DM.19 A body mass index ≥ 30kg/m2 was considered to represent obesity.20 Hypertension was defined as ongoing antihypertensive treatment or systolic blood pressure ≥ 140mmHg and/or diastolic blood pressure ≥ 90mmHg.21 Levels of high-sensitivity CRP were considered to be high in participants with high-sensitivity CRP ≥ 3mg/L.22 Hypercholesterolemia was defined as a total cholesterol concentration ≥ 200mg/dL or treatment with lipid-lowering agents.23 Persons were considered to be smokers if they consumed 1 or more cigarettes per day at the time of the interview.
Statistical AnalysisClusters from Andalusia (Andalusia cohort) and from the rest of Spain excluding Andalusia (Rest of Spain cohort) were analyzed separately. The prevalence of CVRF was calculated in each cohort and was adjusted for the age and sex structure of the Spanish population by the direct method. The prevalence of CVRF in the Andalusia cohort was also adjusted to the Andalusia population age and sex structure. Logistic regression was used to assess the association between geographical area and CVD risk factors, with multiple logistic regression being used to assess the impact of potential confounders on these associations. The logistic regression models were constructed with the geographical area (Andalusia vs rest of Spain) introduced as an independent variable and the presence of CVRF (yes/no) as dependent variables. The corresponding odds ratios (OR) were calculated in models adjusted by age and sex, and also in models that included body mass index/waist circumference. A final model tested the association between the geographical area as the independent variable and the presence of obesity (yes/no) as the dependent variable on a multivariate model that included age, sex, physical activity, educational level, marital status, and working status. These variables were selected as potential confounders because they were associated with obesity in age and sex logistic regression analysis and their frequency was unevenly distributed in the 2 study cohorts (see “Results”). All statistical analyses were performed with SPSS 15.0 and Microsoft Office Excel 2007. Reported P values were based on 2-sided tests with statistical significance set at P < .05.
RESULTSStudy Sample: Andalusia and Rest of Spain CohortsOf the eligible adults selected from the Andalusia centers (3153 after exclusion of listing errors or missing contact data), 54.6% attended the examination, of whom 11.9% were excluded by protocol (institutionalized, severe disease, pregnancy, or recent delivery), giving a final sample of 1517 individuals (mean [standard deviation], age 48.5 [16.1] years; 64.9% women).
Of the eligible adults selected from the rest of Spain (7115 after excluding listing errors or missing contact data),56.0% attended examination, of whom 10.4% were excluded by protocol (institutionalized, severe disease, pregnancy, or recent delivery), giving a final sample of 3586 individuals (mean [standard deviation] age, 51.2 [17.3] years; 53.8% women). There were no differences between the participation rates in the two cohorts (P=.13). The mean age in the Andalusia cohort was lower, and the percentage of women was higher (both comparisons P<.001) than in the rest of Spain.
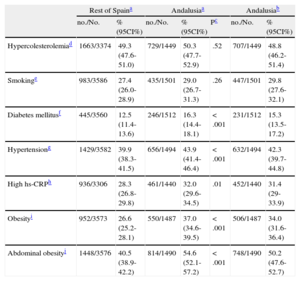
Prevalence of Cardiovascular Risk FactorsTable 1 summarizes the prevalence of age- and sex-adjusted CVRF in both cohorts. In data adjusted to the Spanish population, the proportion of people with DM (P<.001), hypertension (P<.001), high-sensitivity CRP levels (P=.01) and obesity (P<.001) were significantly higher in the Andalusia cohort compared with the rest of Spain. There were also small nonsignificant differences in the prevalence of hypercholesterolemia and smoking. Adjustment of the Andalusia cohort data to the reference population showed only slightly lower prevalences. The greater prevalence of DM, obesity, hypertension and high levels of high-sensitivity CRP in the Andalusia cohort was seen in both men and women and in practically all age groups (data not shown).
Age and Sex Adjusted Prevalence % (95% CI) of Major Cardiovascular Disease Risk Factors by Geographical Area (Andalusia vs Rest of Spain)
| Rest of Spaina | Andalusiaa | Andalusiab | |||||
| no./No. | % (95CI%) | no./No. | % (95CI%) | Pc | no./No. | % (95CI%) | |
| Hypercolesterolemiad | 1663/3374 | 49.3 (47.6-51.0) | 729/1449 | 50.3 (47.7-52.9) | .52 | 707/1449 | 48.8 (46.2-51.4) |
| Smokinge | 983/3586 | 27.4 (26.0-28.9) | 435/1501 | 29.0 (26.7-31.3) | .26 | 447/1501 | 29.8 (27.6-32.1) |
| Diabetes mellitusf | 445/3560 | 12.5 (11.4-13.6) | 246/1512 | 16.3 (14.4-18.1) | <.001 | 231/1512 | 15.3 (13.5-17.2) |
| Hypertensiong | 1429/3582 | 39.9 (38.3-41.5) | 656/1494 | 43.9 (41.4-46.4) | <.001 | 632/1494 | 42.3 (39.7-44.8) |
| High hs-CRPh | 936/3306 | 28.3 (26.8-29.8) | 461/1440 | 32.0 (29.6-34.5) | .01 | 452/1440 | 31.4 (29-33.9) |
| Obesityi | 952/3573 | 26.6 (25.2-28.1) | 550/1487 | 37.0 (34.6-39.5) | <.001 | 506/1487 | 34.0 (31.6-36.4) |
| Abdominal obesityj | 1448/3576 | 40.5 (38.9-42.2) | 814/1490 | 54.6 (52.1-57.2) | <.001 | 748/1490 | 50.2 (47.6-52.7) |
95%CI, 95% confidence interval; hs-CRP: high-sensitivity C-reactive protein.
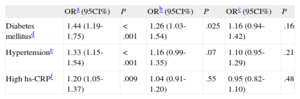
The higher rates of DM, hypertension and high levels of high-sensitivity CRP seemed to be highly associated with differences in adiposity. Logistic regression models adjusted for age and sex showed that the OR of having these CVRF in the Andalusia cohort compared with the rest of Spain cohort were highly significant (P<.001 for differences in DM and hypertension and P=.009 for differences in high levels high-sensitivity CRP. However, after introduction in the regression models of measures of adiposity, such as body mass index and especially waist circumference, the strength of association fell very significantly (Table 2).
Odds Ratios for Diabetes Mellitus, Hypertension and High-sensitivity C-reactive Protein Levels by Geographical Area (Andalusia vs Rest of Spain) in Logistic Regression Models Adjusted for Age and Sex and Adiposity Measurements
| ORa (95CI%) | P | ORb (95CI%) | P | ORc (95CI%) | P | |
| Diabetes mellitusd | 1.44 (1.19-1.75) | <.001 | 1.26 (1.03-1.54) | .025 | 1.16 (0.94-1.42) | .16 |
| Hypertensione | 1.33 (1.15-1.54) | <.001 | 1.16 (0.99-1.35) | .07 | 1.10 (0.95-1.29) | .21 |
| High hs-CRPf | 1.20 (1.05-1.37) | .009 | 1.04 (0.91-1.20) | .55 | 0.95 (0.82-1.10) | .48 |
OR, odds ratio; CI, confidence interval; hs-CRP, high-sensitivity C-reactive protein.
Dependent variable(s): diabetes mellitus (yes/no), hypertension (yes/no), high high-sensitivity C-reactive protein (yes/no).
Independent variable: Andalusia vs rest of Spain.
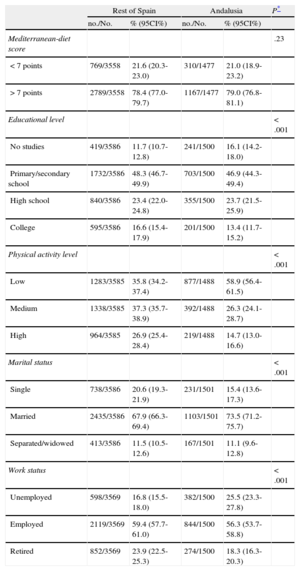
Table 3 compares the prevalence in the Andalusia vs the rest of Spain cohorts of several variables previously selected for their association with obesity by using age and sex adjusted logistic regression analysis.
Comparison of Prevalence (%) of Obesity Risk Factors in Andalusia vs the Rest of Spain
| Rest of Spain | Andalusia | P* | |||
| no./No. | % (95CI%) | no./No. | % (95CI%) | ||
| Mediterranean-diet score | .23 | ||||
| <7 points | 769/3558 | 21.6 (20.3-23.0) | 310/1477 | 21.0 (18.9-23.2) | |
| >7 points | 2789/3558 | 78.4 (77.0-79.7) | 1167/1477 | 79.0 (76.8-81.1) | |
| Educational level | <.001 | ||||
| No studies | 419/3586 | 11.7 (10.7-12.8) | 241/1500 | 16.1 (14.2-18.0) | |
| Primary/secondary school | 1732/3586 | 48.3 (46.7-49.9) | 703/1500 | 46.9 (44.3-49.4) | |
| High school | 840/3586 | 23.4 (22.0-24.8) | 355/1500 | 23.7 (21.5-25.9) | |
| College | 595/3586 | 16.6 (15.4-17.9) | 201/1500 | 13.4 (11.7-15.2) | |
| Physical activity level | <.001 | ||||
| Low | 1283/3585 | 35.8 (34.2-37.4) | 877/1488 | 58.9 (56.4-61.5) | |
| Medium | 1338/3585 | 37.3 (35.7-38.9) | 392/1488 | 26.3 (24.1-28.7) | |
| High | 964/3585 | 26.9 (25.4-28.4) | 219/1488 | 14.7 (13.0-16.6) | |
| Marital status | <.001 | ||||
| Single | 738/3586 | 20.6 (19.3-21.9) | 231/1501 | 15.4 (13.6-17.3) | |
| Married | 2435/3586 | 67.9 (66.3-69.4) | 1103/1501 | 73.5 (71.2-75.7) | |
| Separated/widowed | 413/3586 | 11.5 (10.5-12.6) | 167/1501 | 11.1 (9.6-12.8) | |
| Work status | <.001 | ||||
| Unemployed | 598/3569 | 16.8 (15.5-18.0) | 382/1500 | 25.5 (23.3-27.8) | |
| Employed | 2119/3569 | 59.4 (57.7-61.0) | 844/1500 | 56.3 (53.7-58.8) | |
| Retired | 852/3569 | 23.9 (22.5-25.3) | 274/1500 | 18.3 (16.3-20.3) | |
The percentage of people with a low Mediterranean-diet score did not differ between Andalusia and the rest of Spain. The rest of the variables studied showed some differences: educational level was significantly lower in Andalusia, with significantly more people with no studies and fewer people with a college degree than in the rest of Spain (P<.001). There were also differences in marital status, with fewer single persons in Andalusia (P<.001), and a higher frequency of unemployed persons (P<.001). The reported physical activity level was also clearly lower in Andalusia (P<.001).
In a final logistic regression model, we tested whether these variables could modify the effect of the tendency for the higher risk of obesity in the Andalusia cohort. The OR of being obese in Andalusia vs the rest of Spain was highly significant in logistic regression models adjusted for age and sex (P<.001). However, in multivariate models that also included educational level, marital status, work status, and the degree of physical activity, this effect clearly fell and was no longer significant (P=.086) (Table 4).
Odds Ratios for Obesitya by Geographical Area (Andalusia vs Rest of Spain) in Logistic Regression Adjusted for Age and Sex and Multivariate Models
CI, confidence interval; OR, odds ratio.
Dependent variable: obesity (yes/no).
Independent variable: Andalusia vs rest of Spain.
This nationally representative study shows that the prevalence rates of major CVRF such as obesity, DM, hypertension, and high CRP levels are higher in the region of Andalusia than in the rest of the country, with the results being concordant with the higher CVD mortality rates seen in this region.2 The data suggest that the higher prevalence of obesity in Andalusia seems to be the most decisive factor explaining these differences, in close relation to lifestyle and socioeconomic factors.
The results have special public health implications. The epidemic of obesity, DM and CVD is advancing inexorably all over the world, although its effects may not be the same everywhere, not even within the same country. Thus, the less favored regions socioeconomically may in fact be the most fragile. Andalusia can be considered a less favored region in comparison with the rest of Spain. According to recently updated data, the per capita gross domestic product of Andalusia is the second lowest in Spain (16 960 euros per inhabitant). Moreover, as reflected in our study as well, the percentage of illiterate persons or persons with no studies was higher and the percentage of the population with higher education clearly lower than the national average, whilst the unemployment rate is over 30% (highest in Spain).24 In addition, the per capita public health care budget in Andalusia is currently the second lowest in Spain (1006.38 Euros per protected person, according to the provisional 2013 data).25 This is the setting for the obesity epidemic and its associated CVRF that threatens to impose an extra economic and health care burden on this already less favored region.
The most important result of this study is probably the high rate of obesity in Andalusia. While the national prevalence of obesity (26.6%) and abdominal obesity (40.5%) in Di@bet.es are fairly concordant with those reported in another recent Spanish national survey (22.9% and 35.5%, respectively),26 the obesity prevalence that we found in Andalusia exceeds all the estimates that might have been expected: according to our data, more than one third of adults in Andalusia are obese. These data are comparable to those reported for the United States in the National Health and Nutrition Examination Survey national survey (35.7%),27 a country that ranks number one in the world in obesity prevalence.28 The prevalence of DM in Andalusia also exceeds data reported in most other European countries and the Unites States population.21,29
Geographical variations in the prevalence of CVD and risk factors have been reported in other studies, both between30,31 and within countries.32,33 In Spain too, a north-to-south pattern in CVRF concordant with a similar pattern of CVD mortality have been previously reported.26,34–36 Socioeconomic factors have also been previously associated with geographical variation in obesity and CVD,26,37,38 and our study again highlights the importance of such factors as well as lifestyle (physical activity) in influencing the cardiometabolic risk of a given population. Some other factors, such as health service access and/or quality or other unknown factors cannot be excluded.
Strengths and limitationsThe main strength of this study is the viability of a wide study sampling, representative of the whole national territory with complete sociodemographic and anthropometric information, and analyses performed with a homogeneous methodology, which enabled us to make direct comparisons between data in these cohorts. As limitations, first, the participation was relatively low (54.6% and 56.0% in Andalusia and rest of Spain cohorts, respectively), allowing the possibility of some selection bias. However, the participation rate is similar to other national health surveys performed in European countries39 and in Spain.26 Second, the age and sex structures of the Andalusia and rest of Spain cohorts were not equal. The age difference between the cohorts seems to reflect real differences in the background population.25 Interference of this factor in the results is unlikely since all the prevalence and analytical data were corrected for age and sex. Third, the study was not powered to analyze other regional specific data apart from Andalusia and consequently other regions with a potentially high burden of CVRF could not be analyzed separately.
CONCLUSIONsIn summary, this study contributes information from a national study perspective about the higher prevalence of CVRF in the south of Spain, in close relation with obesity, a sedentary lifestyle, and markers of socioeconomic disadvantage. The results should motivate the health authorities to urgently implement clinical and preventative intervention programs in the region.
FUNDINGThe study was supported by CIBERDEM (Centro de Investigación Biomédica en Red de Diabetes y Enfermedades Metabólicas Asociadas) of Instituto de Salud Carlos III (Ministerio de Ciencia e Innovación), Ministerio de Sanidad y Consumo, Spanish Society of Diabetes and Consejería de Salud Junta de Andalucía (0256/2007). LifeScan Spain (Madrid, Spain) kindly donated the glucometers and test strips for capillary glucose measurements.
CONFLICTS OF INTERESTNone declared.
We wish to acknowledge the kind collaboration of the following entities: The Spanish Diabetes Society, the Spanish Diabetes Federation and the Ministry of Health Quality Agency. Our profound appreciation goes to the primary care managers and personnel of the participating health centers, as well as to Dr. Luis Forga and Dr. Felipe Casanueva for their inestimable help in the management of the northern zone. To all the field workers, nurses and dieticians (I. Alonso, A. Arocas, R. Badia, C.M. Bixquert, N. Brito, D. Chaves, A. Cobo, L. Esquius, I. Guillén, E. Mañas, A.M. Megido, N. Ojeda, R.M. Suarep, M.D. Zomeño), without whose work the study would not have been possible to carry out and to all the people who voluntarily participated in the study.
Sergio Valdés (Centro de Investigación Biomédica en Red de Diabetes y Enfermedades Metabólicas Asociadas [CIBERDEM]; Servicio de Endocrinología y Nutrición, Hospital Universitario Carlos Haya, Instituto de Investigación Biomédica de Málaga [IBIMA], Malaga, Spain), Federico Soriguer (CIBERDEM; Servicio de Endocrinología y Nutrición, Hospital Universitario Carlos Haya, Instituto de Investigación Biomédica de Málaga [IBIMA], Malaga, Spain), Albert Goday (Servicio de Endocrinología y Nutrición, Hospital del Mar, Barcelona, Spain), Anna Bosch-Comas (CIBERDEM; Institut d’Investigacions Biomèdiques August Pi i Sunyer [IDIBAPS], Hospital Clínic de Barcelona, Barcelona, Spain), Elena Bordiú (Laboratorio de Bioquímica, Hospital Universitario San Carlos, Madrid, Spain), Alfonso Calle-Pascual (Servicio de Endocrinología y Nutrición, Hospital Universitario San Carlos, Madrid, Spain), Rafael Carmena (CIBERDEM; Departamento de Medicina y Endocrinología, Hospital Universitario de Valencia, Valencia, Spain), Roser Casamitjana (CIBERDEM; Centro de Diagnóstico Biomédico, Hospital Clínic de Barcelona, Barcelona, Spain), Luis Castaño (CIBERDEM; Unidad de Investigación, Hospital Universitario Cruces, Universidad del País Vasco/Euskal Herriko Unibertsitatea [UPV/EHU], Baracaldo, Vizcaya, Spain), Conxa Castell (Servei d’Educació Sanitària, Generalitat de Catalunya, Barcelona, Spain), Miguel Catalá (CIBERDEM; Departamento de Medicina y Endocrinología, Hospital Universitario de Valencia, Valencia, Spain), Elias Delgado (Servicio de Endocrinología y Nutrición, Hospital Central de Asturias, Oviedo, Asturias, Spain), Joseph Franch (Equipo de Atención Primaria Raval Sud, Institut Català de la Salut, Red GEDAPS [Grupo de Estudio de la Diabetes en Atención Primaria de la Salud], Unitat de Suport a la Recerca, Institut d’Investigació en Atenció Primària Jordi Gol, Barcelona, Spain), Sonia Gaztambide (CIBERDEM; Servicio de Endocrinología y Nutrición, Hospital Universitario de Cruces, UPV/EHU, Baracaldo Vizcaya, Spain), Joan Girbés (Unidad de Diabetes, Hospital Arnau de Vilanova, Valencia, Spain), Ramón Gomis (CIBERDEM; IDIBAPS, Hospital Clínic de Barcelona, Barcelona, Spain), Galde Gutiérrez (CIBERDEM; Unidad de Investigación, Hospital Universitario de Cruces, UPV/EHU, Baracaldo, Vizcaya, Spain), Alfonso López-Alba (Sociedad Española de Diabetes, Madrid, Spain), María Teresa Martínez-Larrad (CIBERDEM; Instituto de Investigación Sanitaria del Hospital Clínico San Carlos [IdISSC], Madrid, Spain), Edelmiro Menéndez (Servicio de Endocrinología y Nutrición, Hospital Central de Asturias, Oviedo, Asturias, Spain), Inmaculada Mora-Peces (Servicio Canario de Salud, Tenerife, Spain), Emilio Ortega (CIBERDEM; IDIBAPS, Hospital Clínic de Barcelona, Barcelona, Spain), Gemma Pascual-Manich (CIBERDEM, Spain), Manuel Serrano-Rios (CIBERDEM; IdISSC, Madrid, Spain), Inés Urrutia (CIBERDEM; Unidad de Investigación, Hospital Universitario de Cruces, UPV/EHU, Baracaldo, Vizcaya, Spain), Jose Antonio Vázquez (CIBERDEM; Servicio de Endocrinología y Nutrición, Hospital Universitario de Cruces, UPV/EHU, Baracaldo, Vizcaya, Spain), Joan Vendrell (CIBERDEM; Servicio de Endocrinología y Nutrición, Hospital Universitario Joan XXIII, Institut d’Investigacions Sanitàries Pere Virgili, Tarragona, Spain) y Gemma Rojo-Martínez (CIBERDEM; Servicio de Endocrinología y Nutrición, Hospital Universitario Carlos Haya, IBIMA, Malaga, Spain).