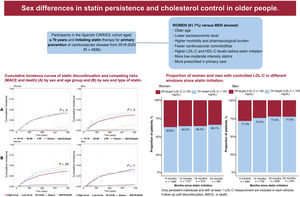
This study aimed to analyze sex differences in statin persistence and associated factors among individuals aged 70 years and older in Spain who initiated statin therapy for primary prevention of cardiovascular disease. Additionally, it assessed the role of sex in low-density lipoprotein cholesterol (LDL-C) control based on the intensity of statin therapy used.
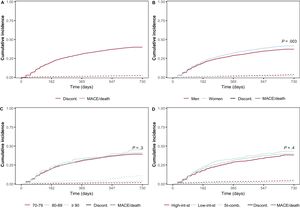
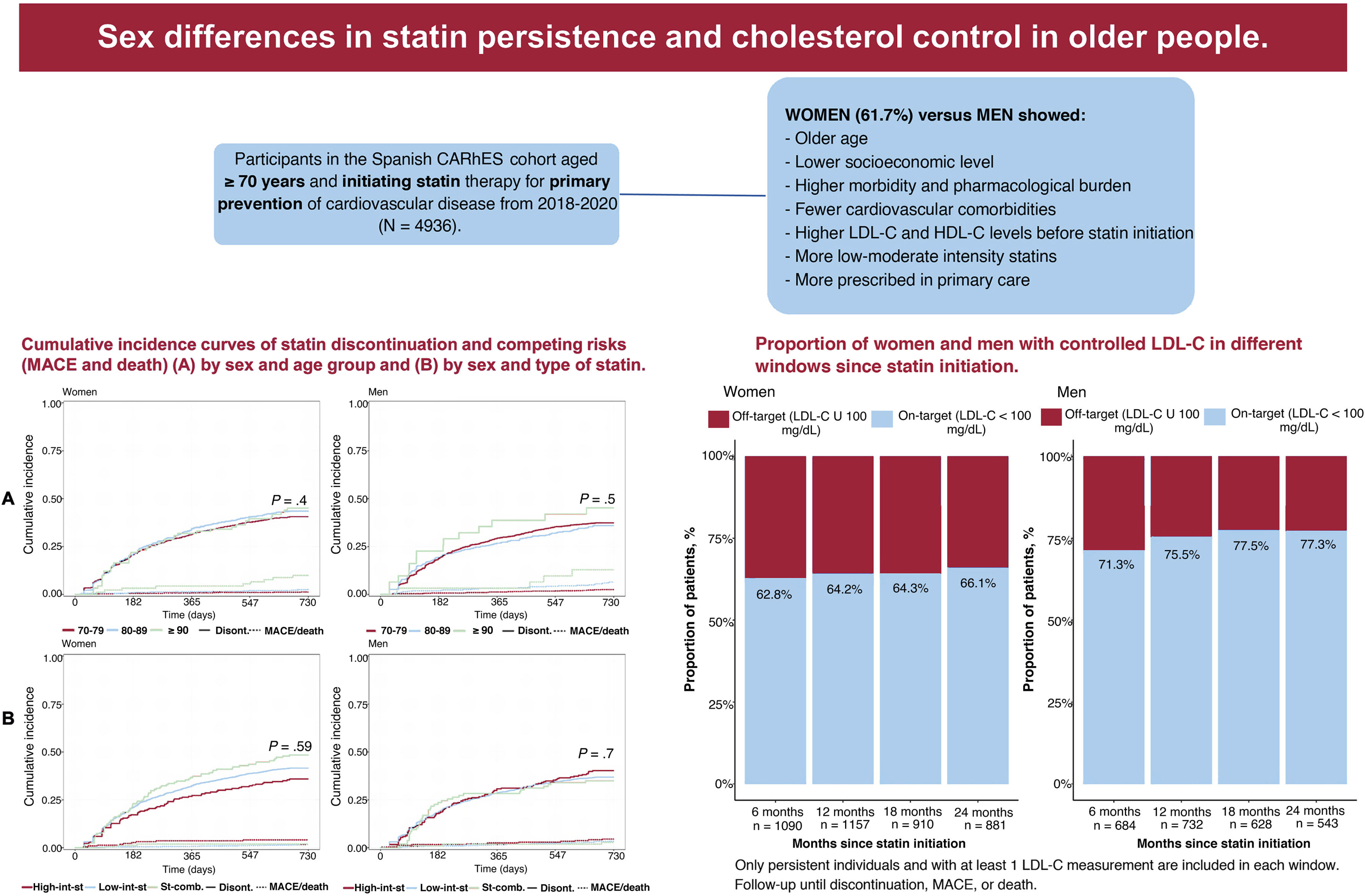
MethodsThis was an observational longitudinal study conducted within the CARhES (Cardiovascular risk factors for health services research) cohort. Individuals aged ≥ 70 years who initiated statin therapy for primary prevention of cardiovascular disease between 2018 and 2020 were included. Two-year statin persistence was assessed by sex. Considering major cardiovascular events and death as competing risks, the risk of statin discontinuation and its associated factors were estimated using cumulative incidence functions and Fine and Gray analysis. The proportion of men and women achieving LDL-C target levels was also calculated.
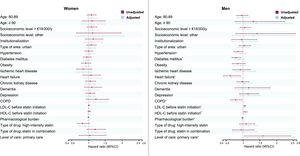
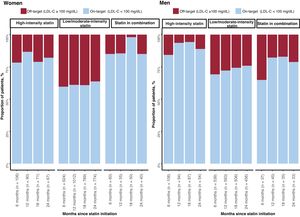
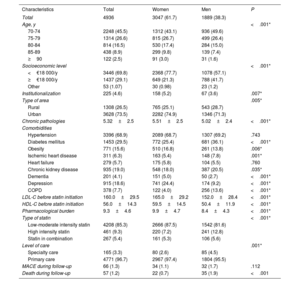
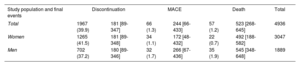
ResultsA total of 4936 older adults (61.7% women) were included. Compared with men, women had higher mean LDL-C levels prior to statin initiation, a greater pharmacological burden, were less likely to receive high-intensity statins, and demonstrated lower persistence. No variables were statistically associated with discontinuation among women. In men, the adjusted HR for discontinuation was 1.03 (95%CI: 1.00-1.06) per 10mg/dL increase in baseline LDL-C level. Among persistent statin users, women were less likely than men to achieve LDL-C targets, particularly when treated with low- to moderate-intensity statins.
ConclusionsSignificant sex differences exist in statin persistence, associated factors, and achievement of LDL-C targets among older adults. These findings highlight the importance of considering sex-specific factors when evaluating the appropriateness of statin use in this population.
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm