
Cardiovascular disease is the leading cause of death worldwide, with an especially devastating impact in low-to-medium income countries. Cardiovascular disease has been elevated to this position by a combination of factors that include urbanization and its attendant effects, such as obesity, a sedentary lifestyle, changes in dietary habits, and smoking. Given the enormous extent of the problem and the complexity of its causes, which include cultural, social, political, and health care factors, an equally sophisticated and comprehensive strategy is required to combat cardiovascular disease on a global scale. Because exposure to cardiovascular risk factors occurs from early ages, this strategy must be expanded and adjusted throughout the life of an individual. Thus, our efforts should be concentrated not only on cardiovascular disease treatment and prevention, but also on health promotion and primordial prevention. In this review, we present different strategies yielding encouraging results at the population level, from childhood until old age, that aim to protect against the challenges facing the scientific community when combating cardiovascular disease.
Keywords
Coronary disease is largely a consequence of lifestyles that are not particularly heart-healthy. Hypertension, obesity, a sedentary lifestyle, smoking, hypercholesterolemia, and diabetes mellitus maintain a direct relationship with the lifestyle of each individual. Recent data show that these life habits are acquired early on in life, specifically at around 3 years to 8 years, and, moreover, that they persist from childhood to adulthood. Thus, promotion of cardiovascular health in childhood represents a great opportunity for primary prevention, particularly in developing countries, which are undergoing considerable changes in health-related behaviors. The structure for implementing these strategies should include school and community programs that promote physical activity and a heart-healthy diet to combat the burden of chronic diseases associated with a sedentary life and obesity.
Cardiovascular health promotion strategies should continue in the transition to adulthood and adjust to the idiosyncrasies of this stage, with the society in which we live exerting a clear deleterious influence on our health. Excessive consumerism and its influence on our habits and behavior, the economic interests of the food industry, the scarce ability of regulatory bodies to influence these characteristics, the growing social and cultural inequalities, and the generally poor communication between the sectors involved in the regulation and monitoring of our health are some of the factors that lead us to live a largely unhealthy life and develop a series of chronic diseases. Faced with this complex structure, and in response to the need to implement strategies that influence the behavior of adult populations, a new approach has been initiated to improve population-wide cardiovascular risk profiles by using community help and communication programs that involve adults helping each other, with a methodology similar to that of other organizations (such as Alcoholics Anonymous).
Health promotion must include the oldest population of our society. Atherosclerosis is a ubiquitous process that affects almost all of the human body, and there is increasing evidence of the pathological link between coronary disease and neurodegenerative disease (NDD). The NDD has become a major health problem, together with population aging and the global burden of cardiovascular disease (CVD). Recent research has provided solid evidence on the association between the risk of Alzheimer disease (AD) and dyslipidemia, a sedentary lifestyle, hypertension, obesity, diabetes mellitus, and smoking. This association indirectly identifies atherosclerosis and coronary disease as significant etiological factors for degenerative cerebral disease. Accordingly, studies must determine if intervention programs aimed at multiple risk factors and that encompass different life stages of individuals effectively delay the onset and progression of symptomatic dementia.
Therefore, we believe that if we want to affect population health, we must implement strategies that facilitate the acquisition and maintenance of heart-healthy habits that are adapted to the specific needs of the different life stages, from childhood to old age. Only via coordinated strategies for health promotion and cardiovascular prevention throughout an individual's life will we succeed in counteracting the increase in CVD.
CARDIOVASCULAR HEALTH PROMOTION IN CHILDHOOD: THE SI! (SALUD INTEGRAL) PROGRAMThe preclinical substrate of atherosclerotic disease (lipid material) begins at early ages and its development largely depends on nonheart-healthy behavior that determines exposure to risk factors. Low exposure of adults to risk factors is associated with a decrease in cardiovascular death, increase in survival, and improved quality of life.1
Population studies have revealed the importance of health promotion, primordial prevention (defined as preventing the adoption of risk factors), and primary prevention (which combines interventions aimed at modifying risk factors to prevent an initial cardiovascular event).2 Particularly worrying are trends that show not only increased levels of obesity and diabetes mellitus, but that these diseases develop at younger and younger ages.3 These trends underline the need to adopt health promotion strategies that include primordial and primary prevention programs that are implemented throughout an individual's life.
During recent decades, the main cardiovascular risk factor in both adults and children has been identified as obesity and associated factors, such as diabetes mellitus and hypertension, a consequence of inadequate nutrition and limited physical activity. Recently, results have been published on the incidence and prevalence of childhood obesity in the United States, with 12.4% and 14.9% of preschool-aged children obese and overweight, respectively.4 Spanish children currently have largely unhealthy habits such as poor nutrition and inadequate physical activity, which are causing a high prevalence of childhood obesity. In Spain, the prevalence of overweight and obesity in the population aged 2 years to 24 years was 26% in 2000. The prevalence of obesity (14%) was higher in males (16%) than in females (12%).5 Boys and girls from 6 years to 13 years showed higher rates of obesity. Obesity is more prevalent at lower socioeconomic and education levels. In Europe, the highest prevalence of obesity was seen in southern countries, with 36% and 31% of children either overweight or obese in Italy and Greece, respectively.6 The risk factors of CVD, typically studied in adult populations, can already be seen in the Spanish childhood population. Addiction to alcohol, tobacco, and other drugs are also important risk factors for CVD, and Spanish children have high levels of addiction to substances such as tobacco and alcohol.7 In 2008, an epidemiological study performed in 14-year to 18-year-old students revealed that 81.2% and 44.6% had previously consumed alcoholic drinks or tobacco, respectively.8
Data obtained via noninvasive imaging studies have shown that exposure to cardiovascular risk factors (CVRFs) during childhood and adolescence is associated with a significant increase in subclinical atherosclerosis during adulthood.9 For example, the Young Finns study found that exposure of adolescents aged 12 years to 18 years to risk factors predicted a significant increase in carotid intima-media thickness in adulthood.10 These population studies have provided additional evidence on the need to begin primordial prevention and cardiovascular health promotion at early ages. These studies have shown high prevalence of the main CVRFs in childhood11–13 and, moreover, that these risk factors are potentially modifiable.14,15 These data have led to the development of clinical guidelines on primordial and primary prevention in children and adolescents.16,17
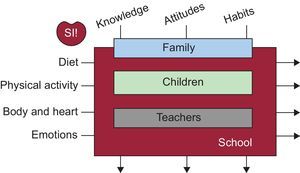
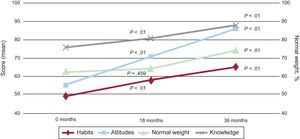
Thus, we believe that there is an urgent need to implement high-quality health education programs for children (both for families and in the school environment), to help them to adopt heart-healthy lifestyles that are maintained in their transition to adolescence and adulthood. Thus, a total health program called SI! (salud integral [comprehensive health]) has been designed to promote cardiovascular health in children from 3 years to 5 years, strengthening healthy behavior to modify CVRFs. Using the school environment and drawing on the teaching experience of Sesame Street and its tradition of high-impact educational programs, this program is introducing a conceptual change in disease prevention by moving toward health promotion. In the implementation of this type of intervention, the school environment plays a fundamental role, given that it provides an appropriate environment for evaluating the effectiveness of an intervention in controlled conditions. Moreover, the most effective interventions introduced in schools are those that involve families and have as an objective behavioral markers such as changes in knowledge, attitudes, and habits.18,19 Following this strategy, a first study was performed in Bogotá (Colombia), including 1216 children, 928 families, and 120 teachers who were observed for 3 years following randomization of participating schools to receive a 6-month intervention for promoting cardiovascular health.20 The results were impressive, and significant improvements were found in all indexes of knowledge, attitude, and habits in the schools that received the intervention. Furthermore, these differences were maintained for 36 months after the intervention, indicating the persistence of the heart-healthy habits that are acquired at this age (Figure 1).21
![Diagram of the implementation of the SI! (Salud Integral [comprehensive health]) program.](https://static.elsevier.es/multimedia/18855857/0000006700000009/v1_201408291224/S1885585714002072/v1_201408291224/en/main.assets/gr1.jpeg?xkr=eyJpdiI6Im5QSURmUXUrS3BIL0dJaG1RVEpSQUE9PSIsInZhbHVlIjoiaGRTQVl4V003cWtaS3BnTWJCMnI4RHRoeTFTSlRqS2F2cEJXejExeHF5QjdKMXpFT0V0bkVGYWNadG9mSkcwSXE0Ylo2N01BK0hWU2U1WlNQYTRqM0U2czgxc2x2ZVFCU2JDbDNtTzNMNVhVVE9aQWFzd3VCYWhpRzJGejRNbnJzU3Q5Sm9KZUVhVW9IRDdwemRTZzdISVAyWDVWS04xU3ZlQys3Y2FZRlV0ampxNXRCVlFMUlZBeXRXYng4dE9LOEFIalVYajZUMkk1UFZoSXNPYWVISmF6NkNNSUFNZXpPa0dJbG1ab2RxVzhpb3BHN3BRUXc1WGZJV1JkYlIzdTBGWHVLSUYrR3RrYTFrSzRwYlIxYi94dmFXdnZ5MFJaZmFBVlV2Nk5Cbmc9IiwibWFjIjoiODkzMmJhNTk2YTJlNzIwYWQ2OGQxZDVkMzI3ODRhNTVhOGViZjcxNjVlYjM5YjBiNTQ3NzlmMWNkZjFiMWJkNSIsInRhZyI6IiJ9 "Diagram of the implementation of the SI! (Salud Integral [comprehensive health]) program.")
Considering the main CVRFs and following a total health promotion approach that goes beyond obesity prevention, the SI! program is directed at children from 3 years to 16 years old and aims to establish healthy lifestyles at an early age by intervening in 4 basic inter-related components: the human body, physical activity, diet, and, for the first time and expanding on the original design, management of emotions as a fundamental component of behavior aimed at preventing the use of harmful substances, such as tobacco, alcohol, and drugs. These components are studied in 3 dimensions, each corresponding to an evolving concept: knowledge, attitudes, and habits. Thus, individuals go from understanding the component (knowledge) to its practice (attitude), and to the acquisition of a pattern of behavior that is maintained over time (habit) (Figure 2).

Thus, and based on our experience with the SI! program, there are different basic elements for the successful implementation of a health promotion program based in the school environment: a) preschool-aged children (beginning at 3 years) as the target population, which encompasses other users (parents, teachers, and schools); b) an approach involving 4 educational components: human body, diet, physical exercise, and emotions; c) use of new technology and interactive activities to involve family members; d) integration of a school environment-based program into the academic curriculum; e) effectiveness evaluation, which includes repetition of the model in different countries via clinical trials, and f) assessment of program cost-effectiveness to promote its adoption among local governments.
The program is based on didactic material and educational strategies such as the characters of Sesame Street, which are used for this purpose in the projects in Colombia and Spain. Moreover, it is constantly appraised by specialists in medicine, childhood development, and communication to improve the validated strategies applied. An important point of the program is the persistence of the effect. To demonstrate that the effect of the intervention is persistent, the impact of the program is evaluated at different stages of the intervention via measurements of health determinants, which include a range of indicators, from basic changes in behavior (knowledge, attitude, habits) to intermediate clinical markers (body mass index).
The final objective of any health promotion program is a reduction in the mortality and comorbidity of a population, an increase in the quality of life during adulthood, and a decrease in associated health care costs. By acting on the behavior of preschool-aged children, we hope to avoid the acquisition of habits that expose them to CVRFs at a young age. Even modest improvements in the cardiovascular risk profile will have a marked impact on the adults of the future, given the prevalence of the problem and the developmental time of the disease.
ADULT BEHAVIORAL INTERVENTIONSGrenada Heart StudyThe Grenada Heart Study resulted from conversations between the principal investigator and a panel of representatives from the United Nations concerned by the imminent CVD epidemic who were looking for a suitable model in countries with limited incomes.
Located in the Caribbean Sea, the island of Grenada has a population of 104 487, the majority of African descent. Because the island has recently undergone a process of Westernization, it currently has rates of hypertension and diabetes mellitus that are higher than those seen in the United States. In contrast, the paradoxically low prevalence of CVD supports the view that the country is undergoing an obesity-related “risk transition”. This phenomenon usually results when there is a disproportionate increase in obesity-related diseases due to an increase in smoking and excessive intake of fat and alcohol, generally in the context of a rapid urbanization that particularly affects middle-aged individuals.22 In the case of a country such as Grenada that has limited resources, the potential increase in CVD combined with a high rate of infectious diseases saddles the country with a “double burden” of disease, which could have catastrophic consequences for population health. Although the risk transition is almost complete, the transition corresponding to cardiovascular morbidity and mortality remains to be seen, which presents a rare opportunity for prevention to achieve CVRF control and eliminate the future burden of the disease.
This ongoing study is based on reinforcing habits proven, with excellent results, to be healthy and, moreover, has shown that the active participation of health care professionals is dispensable. In this case, the entire population of the island was divided into groups with the aim that some participants would help others to achieve various lifestyle targets, such as diet changes, weight loss, optimal blood pressure, and regular physical exercise.23 This model has allowed implementation of an efficient local monitoring system that has revealed important information on the changes necessary for controlling CVD, particularly in environments with limited resources.
Cardona Integral Fifty-Fifty ProgramDeveloped from the experience of the island of Grenada, the aim of the Fifty-Fifty program is to improve the overall health of 25-year to 50-year-old adults by helping them to improve their health habits and manage their main risk factors for CVD: excess weight and obesity, a sedentary lifestyle, smoking, and hypertension. The program is being performed in various Spanish towns in collaboration with the Spanish Federation of Municipalities and Provinces (Federación Española de Municipios y Provincias), and is derived from the SHE (Science Health and Education) Foundation initiative, fostered by Dr. Valentín Fuster, and of the Spanish Agency of Food Safety and Nutrition (Agencia Española de Seguridad Alimentaria y Nutrición) of the Spanish Ministry of Health, Social Services and Equality (Ministerio de Sanidad, Servicios Sociales e Igualdad), in the framework of the NAOS (acronym of Nutrición, Actividad física, prevención de la Obesidad y Salud [nutrition, physical activity, obesity prevention and health]) strategy and of the Observatory of Nutrition and Study of Obesity (Observatorio de la Nutrición y de Estudio de la Obesidad). The main objective of the Fifty-Fifty program is to improve the overall health of adults by modifying their health habits.
Fifty-Fifty is implemented through training and motivational workshops, with all participants in the program receiving 10h of training directed at promoting healthy life habits. During the subsequent 12 months, this training is accompanied by role playing aimed at promoting internal changes and providing participants with the possibility of developing abilities that transcend simple knowledge to help them to better themselves (Figure 3).

In Cardona (Spain), the Fifty-Fifty program expands on the original pilot study, and includes an ambitious urban plan designed to provide an environment that promotes physical activity in a population. The idea is to incorporate healthy habits into daily life through an urban environment design that facilitates and promotes these habits. Through the promotion of an active lifestyle, the project encourages individuals to make healthy decisions on how they move around, what they eat, and how they interact with their surroundings. The program transcends the health care field and includes, for example, projects aimed at recovering natural environments with the participation of volunteers from Cardona and integration of unemployed locals into the project according to their specific abilities, as well as conversion of reading spaces in the municipal library. The Cardona Integral Fifty-Fifty program attempts to be a model that inspires the creation of healthy towns that help their inhabitants to choose and maintain healthy ways of life.
VASCULAR DISEASE IN OLD AGE: RELATIONSHIP WITH DEGENERATIVE DISEASEAtherosclerosis is an omnipresent disease that affects almost the entire arterial tree. One of the more representative examples of the systemic nature of atherosclerosis may be the relationship between coronary disease and NDD, whose main manifestation is dementia.
Dementia includes AD, vascular dementia, and poststroke dementia. Although AD is the form of dementia that is most frequently diagnosed in the older population, the cognitive alterations caused by vascular disease, such as subclinical cerebral damage, silent cerebral infarction, and stroke, are important and independent causes of dementia that significantly contribute to cognitive dysfunction. Estimations of the prevalence of NDDs have increased in parallel with the general aging of the population, and they have become a public health priority due to their effect on morbidity and mortality and their considerable economic impact. The Delphi 2 study estimated a prevalence of 24.3 million people worldwide diagnosed with dementia in 2001, and projected that this number would increase to 42.3 million in 2020 and 81.1 million in 2040.24 The countries or regions with a higher number of affected individuals are China and the Western Pacific, Western Europe, and the United States.25
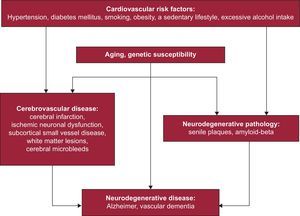
In recent years, a paradigm shift has been seen in the pathological processes that underlie the development of dementia, with data showing that CVRFs dramatically increase the risk of NDDs. Accordingly, there are associations between the risk of AD and dyslipidemia/hypercholesterolemia,26 a sedentary lifestyle,27 hypertension,28 obesity,29 diabetes mellitus type 2,30 and smoking.31 The evidence supporting the etiological role of CVRFs in the development of AD is consistent, particularly when it is evaluated from a longitudinal perspective that spans an individual's life (Figure 4).

Two epidemiological studies have provided solid evidence on the association between CVRFs and dementia. The Honolulu-Asia Aging Study found a strong correlation between the risk of dementia and hypertension present in middle age in a cohort of 3703 male Americans of Japanese origin.32 The risk of dementia was almost 5 times greater in patients with a systolic blood pressure of 160mmHg than for those at between 110mmHg and 139mmHg (relative risk = 4.8; 95% confidence interval, 2.0-11.0). The Rotterdam Study found a similar correlation with diabetes mellitus in 6370 older patients, with almost double the risk of dementia (relative risk = 1.9; 95%CI, 1.3-2.8) of those without diabetes.30
Moreover, improvements in neuroimaging techniques have revealed that a substantial proportion of patients clinically diagnosed with AD have no detectable deposits of amyloid beta (Aß) in the brain (which has been termed suspected SNAP [non-amyloid pathology]). This proportion reaches 30% of that population in some clinical trials.33 The question that emerges from this observation is obvious: what pathological process, apart from Aß deposition, governs the onset of dementia in this group of patients? To try to clarify the relationship between cerebrovascular damage and Aß deposition and their associations with cognitive ability, Marchant et al34 used neuroimaging techniques (magnetic resonance and PiB-PET [Pittsburgh Compound B positron emission tomography]) and cognitive tests to study a population of older persons with a high cardiovascular risk profile and various degrees of cognitive alterations. In this population, cerebrovascular damage was shown to be more important than Aß in cognitive function, maintaining a predictive ability even after adjusting for the influence of Aß deposition. This finding demonstrates the importance of cerebrovascular damage in cognitive alteration and indicates a significant impact of cerebrovascular diseases on the etiology of cognitive alterations.
In relation with the role of the CVRFs, the higher risk of dementia in the middle-aged population has been attributed to hypertension (up to 30% of dementia cases). Moreover, based on epidemiological data, diabetes mellitus confers a high risk of dementia.35 Therefore, vascular and metabolic factors should be considered indispensible objectives for preventing dementia. The timing of these interventions is critical, given that the association between dementia and CVRFs appears to be stronger during middle age and weaker in later life stages, which indicates that these interventions should be made decades before disease onset. Thus, given that the most common forms of dementia become apparent in the older population, even small delays in the onset or worsening of cognitive decline could result in significant reductions in the incidence of the disease. For example, it has been estimated that of the 106 million cases of AD that are predicted in 2050, around 23 million could be completely avoided if preventive interventions were able to delay disease onset by 2 years.36 Moreover, safeguarding normal cognitive development during childhood and adolescence based on the importance of these factors in later life stages is a requirement for any program to prevent cognitive alteration.37 Thus, the importance of a balanced diet in earliest stages of development has been widely recognized as a fundamental factor in neurocognitive development.38
The lack of success of the majority of preventive and therapeutic trials underscores the need to develop new strategies for future studies. In particular, new intervention programs should be designed to encompass the entire life span and consider the multifactorial nature of NDD. Theoretically, given that the CVRFs are involved in the pathogenesis and clinical expression of NDDs, intervention programs aimed at promoting health and modifying CVRFs should effectively postpone the onset of dementia and reduce the overall burden of symptomatic NDD.
CONCLUSIONSCardiovascular disease is complex and responds to different risk factors, most of which are modifiable and acquired in the earliest stages of life. Once behaviors are acquired, they are carried over to adulthood. Modern society has developed environments that typically fail to help individuals to acquire and maintain heart-healthy life habits. All of these factors have led to the adoption of new intervention models that aim to facilitate heart-healthy and persistent behavior from childhood. In adulthood, the combined strategy of a novel intervention model in which small intervention groups become responsible for helping each other and where urban spaces are designed to facilitate the acquisition of healthy habits is showing promising results in entire populations. Finally, the relationship between CVRFs and NDD is undoubtedly closer than suspected. Thus, it is imperative to study if intervention programs aimed at multiple modifiable risk factors from a longitudinal perspective that span different life stages of individuals effectively delay the onset and progression of symptomatic dementia.
CONFLICTS OF INTERESTSNone declared.