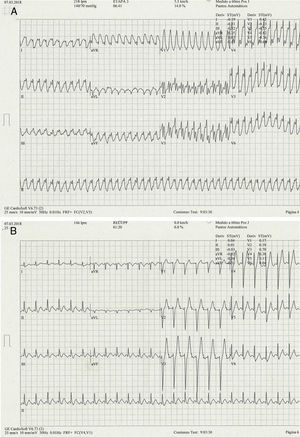
Diagnostic certainty in these tachycardias is not possible with the 2 main differential diagnostic algorithms (Figure 1A), given that they yield different results: the Brugada algorithm suggests a process with a ventricular origin whereas the Vereckei one points to a supraventricular origin; therefore, responses 1 and 2 are incorrect.1

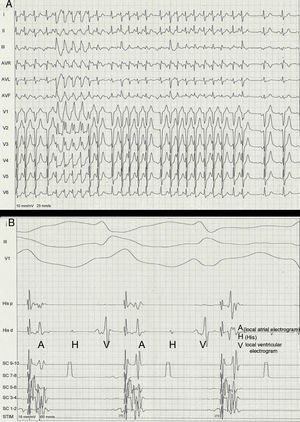
Figure 1B shows the ECG after resolution of the tachycardia. This is consistent with atrial flutter with 2:1 atrioventricular conduction and common atrial flutter with F wave morphology/polarity. During atrial stimulation with isoproterenol, electrophysiological study showed his-Purkinje axis aberrancy with a QRS complex very similar to that of the tachycardia (Figure 2A). The supraventricular origin was confirmed by the intracavitary electrogram (Figure 2B). Therefore, this is a 1:1 conduction atrial flutter with right branch and left bundle branch aberrancy, causing right shift of QRS axis (response 3 is incorrect, response 4 is correct). The cavotricuspid isthmus was successfully ablated.
