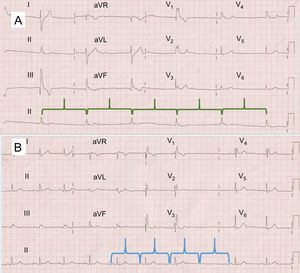
The original electrocardiogram (ECG) performed in the emergency department revealed the presence of wide QRS sinus bradycardia without atrial activity (Figure A), requiring a differential diagnosis involving atrial fibrillation with complete atrioventricular block or complete sinoatrial block (SAB), which are indistinguishable on surface ECG. Discontinuation of digoxin therapy resulted in sinus rhythm with a second-degree Mobitz SAB. This conclusion is based on the observation that the P-P interval of the pause is exactly twice as long as the preceding P-P interval and that the P wave-QRS complex prior to the pause does not arrive early, as would be the case with supraventricular premature complexes (Figure B). This supports the diagnosis of complete SAB in the original ECG (correct response: option 3).

The effect of digoxin on the sinus node is a subject of debate, but there have been reports of a decrease in sinus node rate, an increase in sinus node recovery times, and SAB.1,2