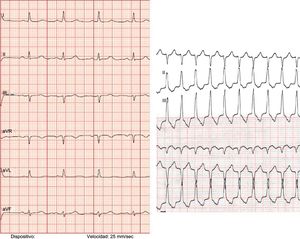
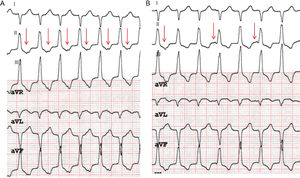


The ECG recording during tachycardia shows a longer QRS interval than in sinus rhythm (115ms). There are differences in the QRS morphology of tachycardia (90° axis during tachycardia vs 30° in sinus rhythm; negative complex in leads I and aVL in tachycardia vs positive complex in sinus rhythm) without meeting the criteria for aberrant conduction (Figure 1). Supraventricular tachycardia is ruled out (answers 1 and 2, incorrect). Prior to adenosine administration, a notched T wave can be observed in the lower leads, which could correspond to an atrial mechanism. An atrial/ventricular ratio of 1:1 is observed (Figure 2A). After adenosine administration, which interrupts ventriculoatrial conduction, atrioventricular dissociation can be observed (Figure 2B), confirming that this is ventricular tachycardia with 1:1 ventriculoatrial conduction (there is an effect of adenosine on the tachycardia but without conversion to sinus rhythm, thus ruling out option 3). The correct answer is therefore number 4: the electrophysiological diagnosis was idiopathic right ventricular outflow tract tachycardia.
ISSN: 1885-5857
Impact factor 2024
4.9