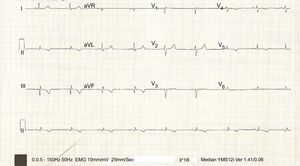
The patient had regular tachycardia with a QRS of 120ms, right superior axis, and right bundle branch blockage; the postcardioversion electrocardiogram is shown in the Figure. Based on the previous infarction, morphological criteria, and right superior axis, supraventricular tachycardias can largely be ruled out (responses 1 and 3). Patients with previous infarction and septal involvement can show ventricular tachycardias with a relatively narrow QRS due to invasion of the His-Purkinje system.1 Although the same history makes posterior fascicular ventricular tachycardia unlikely, an electrophysiological study is required for their differentiation (response 2). In this study, tachycardia was induced, similar to the clinical tachycardia, by intramyocardial reentry related to an inferoposterior septal scar, with a septal exit close to the left branch of the bundle of His (response 4). The mechanism was confirmed by the success of the ablation.

Clinical practice guidelines recommend defibrillator implantation in patients with ventricular tachycardia and previous infarction.2 In some patients, an electrophysiological study can be useful to clarify mechanisms that would respond to ablation.