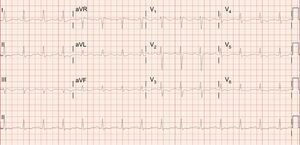
The correct answer is option 4. The patient admitted to having taken at least 800mg of flecainide. She underwent gastric lavage and received activated charcoal and a sodium bicarbonate infusion, and she improved clinically. Repeat ECG showed an RS complex, a long PR interval, and narrowing of the QRS, still with right bundle branch block (Figure), which corrected completely hours later.

Supraventricular tachycardia with aberrant conduction (option 2) could be ruled out because with the patient's paroxysmal atrial fibrillation with rapid ventricular response she maintained a narrow QRS. Massive pulmonary embolism (option 3) could be excluded due to the progressive narrowing of the QRS and the absence of risk factors. Interestingly, flecainide toxicity usually produces prolongation of the PR interval, hampering identification of P waves, and progressive widening of the QRS along with prolongation of the QT interval,1 which hampers the the differential diagnosis with ventricular tachycardia2 as it meets the criteria on several algorithms (option 1, incorrect). In this case, the relatively slow rate of the tachycardia along with the QT prolongation help make the diagnosis.