Despite the established role of cardiac resynchronization therapy (CRT) in patients with heart failure (HF),1,2 researchers remain active in understanding the benefit of this therapy and exploring new indications. One important issue is the highly variable response rate to CRT and the identification of effective responders.3
Response to CRT also has a wide range of terminology, including mid-term left ventricular (LV) reverse remodeling, symptomatic improvement, reduction of HF events/mortality, or a combination of these parameters. Depending on the definition of response, nonresponse to CRT occurs in 30% to 45% of patients. On the other hand, dramatic favorable response occurs in a subset of patients, characterized by significant improvement of LV ejection fraction (LVEF) with reverse remodeling leading to normal or near normal recovery of cardiac function, a condition now referred as “super-responders” to CRT.
As super-responders are characterized by significant improvement of LVEF, to near normalization, a new question arises on whether these patients continue to require CRT with defibrillator (CRT-D) upon device replacement, i.e., whether a CRT with pacemaker (CRT-P) downgrade will be sufficient. As LVEF is the single most important predictor of sudden cardiac death, a post-CRT value well above 40% or even close to 50% may imply that the subsequent risk of sudden cardiac death will be low. For patients who received a defibrillator for primary prevention, theoretically a downgrade from CRT-D to CRT-P will render the therapy more cost-effective, especially in the elderly population. Understanding the relationship between the degree of CRT response and the reduction of risk of ventricular arrhythmias will shed light on this important clinical issue.
In an article published in Revista Española de Cardiología, García-Lunar et al4 reported the results of a retrospective analysis of 196 HF patients who received CRT-D and compared the incidence of ventricular arrhythmias in different subgroups according to the degree of echocardiographic response. Patients were enrolled according to previously established CRT guidelines. Ventricular arrhythmias were assessed as any episode detected by the defibrillator that required antitachycardia pacing or defibrillation therapy. Super-responders were defined as a 2-fold or greater improvement in LVEF or a final LVEF ≥ 45% at 12 months post-implantation.
The authors found a 78.2% and 80.8% reduction of ventricular arrhythmias in super-responders, compared with responders (increase in LVEF ≥ 5%) and nonresponders, respectively. Further analysis showed that independent predictors of ventricular arrhythmias were the lack of super-response to CRT, secondary-prevention device implantation, amiodarone treatment, and QRS > 160ms.
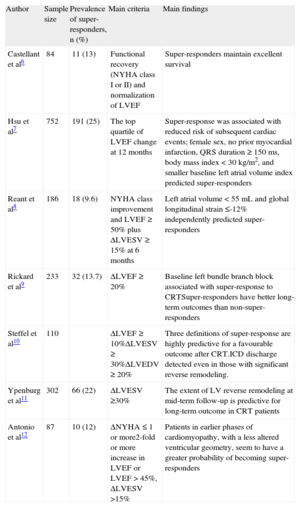
The improvement of LVEF and achievement of LV reverse remodeling by CRT is far greater than that of medical therapy for HF. While neurohormonal blockers antagonize traditional factors governing the pathophysiological mechanisms of HF, CRT primarily corrects the poor timing of contraction as a result of electromechanical delay.5 Nonetheless, there is a subset of patients who are super-responders to CRT. Previous studies reported a highly variable prevalence of super-responders, ranging from 9.7% to 29%.6–12 Such variation is likely related to differences in criteria used to define super-responders, which applied different echocardiographic and/or clinical parameters (Table). A commonly used clinical parameter is New York Heart Association functional class, which is limited by its subjectivity and significant placebo effect, as observed in randomized, controlled trials.1,2 Furthermore, LV end-systolic volume was used in most of the previous studies as a major criterion for responders instead of LVEF, as it represents a combined effect of increase in systolic function and reduction of LV mass, both of which are hallmark features of LV reverse remodeling. Typically, super-responders have been described as more likely occurring in nonischemic etiology with complete left bundle branch block, and possibly in women.13 In the current study, the only difference observed in super-responders was the higher prevalence of nonischemic etiology.
Main Studies Assessing Super-responders After Cardiac Resynchronization Therapy
| Author | Sample size | Prevalence of super-responders, n (%) | Main criteria | Main findings |
| Castellant et al6 | 84 | 11 (13) | Functional recovery (NYHA class I or II) and normalization of LVEF | Super-responders maintain excellent survival |
| Hsu et al7 | 752 | 191 (25) | The top quartile of LVEF change at 12 months | Super-response was associated with reduced risk of subsequent cardiac events; female sex, no prior myocardial infarction, QRS duration ≥ 150ms, body mass index < 30 kg/m2, and smaller baseline left atrial volume index predicted super-responders |
| Reant et al8 | 186 | 18 (9.6) | NYHA class improvement and LVEF ≥ 50% plus ΔLVESV ≥ 15% at 6 months | Left atrial volume < 55mL and global longitudinal strain ≤-12% independently predicted super-responders |
| Rickard et al9 | 233 | 32 (13.7) | ΔLVEF ≥ 20% | Baseline left bundle branch block associated with super-response to CRTSuper-responders have better long-term outcomes than non-super-responders |
| Steffel et al10 | 110 | ΔLVEF ≥ 10%ΔLVESV ≥ 30%ΔLVEDV ≥ 20% | Three definitions of super-response are highly predictive for a favourable outcome after CRT.ICD discharge detected even in those with significant reverse remodeling. | |
| Ypenburg et al11 | 302 | 66 (22) | ΔLVESV ≥30% | The extent of LV reverse remodeling at mid-term follow-up is predictive for long-term outcome in CRT patients |
| Antonio et al12 | 87 | 10 (12) | ΔNYHA ≤ 1 or more2-fold or more increase in LVEF or LVEF > 45%, ΔLVESV >15% | Patients in earlier phases of cardiomyopathy, with a less altered ventricular geometry, seem to have a greater probability of becoming super-responders |
CRT: cardiac resynchronization therapy; ICD: implantable cardioverter defibrillator; LVEDV: left ventricular end-diastolic volume; LVEF: left ventricular ejection fraction; LVESV: left ventricular end-systolic volume; NYHA: New York Heart Association.
Despite the lack of a unifying definition, previous studies have consistently demonstrated that CRT super-responders had favorable long-term prognosis.6–12 This observation corroborates the hypothesis that mid-term LV reverse remodeling and gain in LVEF predicts a favorable long-term prognosis in terms of lower all-cause and cardiovascular mortality as well as HF events.5,14 Previous studies had observed a reduction of ventricular arrhythmias in CRT super-responders.15,16 On the other hand, appropriate implantable cardioverter-defibrillator discharges occurred in super-responders despite a reduction in ventricular arrhythmias.10 So the clinical question is: Should CRT-D be downgraded to CRT-P in super-responders to CRT?
From the published data, it is apparent that CRT-D will be necessary upfront when CRT is provided as a new therapy, as these patients had LVEF < 35%, even in the setting of primary prevention of sudden cardiac death. However, over the course of a few years when patients develop significant LV reverse remodeling response with near normalization of LVEF, the subsequent risk of ventricular arrhythmias will be minimized. Therefore, although CRT-D may be necessary to prevent sudden arrhythmic death in the first few years of treatment, such need should be reviewed at the time of device replacement in the super-responders. In fact, the use of CRT-P alone also reduced sudden cardiac death in the CARE-HF study.14 In the current study, although 3 patients in the super-responder group developed ventricular arrhythmias, it is not known whether these patients had indications for a defibrillator as secondary prevention of sudden cardiac death (occurred in 9 out of 51 patients) or were put on amiodarone due to history of arrhythmias (occurred in 13 out of 51 patients). Furthermore, the current study is a retrospective analysis of patients over a period of 13 years, and there was a significant amount of incomplete data, leading to a high proportion of patients being excluded from analysis. Therefore, in order to determine the best balance between efficacy and cost-effectiveness of the second device in CRT super-responders, it is imperative to conduct a randomized trial that compare CRT-P downgrade and continuation of CRT-D in patients without an implantable cardioverter-defibrillator indication at the time of device replacement. There are 2 further practical considerations. The first is how to draw a line to define the cutoff value for super-responders and what parameters it should be based on. One possible criterion is significant LV reverse remodeling (e.g. > 30% reduction of LV end-systolic volume) and LVEF > 45%. The other issue is that patients with ischemic etiology may have progression of coronary heart disease, and hence, high risk of further ischemic events that will further impair LVEF. In such patients, a short-term CRT-P downgrade at the time of device replacement may not be advisable.
CONFLICTS OF INTERESTNone declared.