
Understanding the societal impact and trends of coronary heart disease through basic epidemiological measures is essential to evaluate treatment effectiveness and organize resource distribution. In the following narrative review, data are presented on the prevalence, incidence, and prognosis of coronary heart disease in general and of acute coronary syndrome in particular.
Keywords
Although the mortality rate from ischemic heart disease has decreased in the last 4 decades in developed countries, it continues to cause approximately one third of all deaths in persons older than 35 years of age.1 It has been estimated that almost half of middle-aged men and one third of middle-aged women in the United States will have some symptoms of ischemic heart disease.2 Meanwhile, cardiovascular disease causes an estimated annual total of 4 million deaths in Europe and of 1.9 million deaths in the European Union, largely due to coronary heart disease (CHD),3 representing 47% and 40% of all deaths in Europe and the European Union, respectively. In Europe, cardiovascular disease leads to a total estimated annual cost of 196 billion euros of which approximately 54% is due to direct health care costs and 24% is due to lost productivity. Moreover, the effects of CHD are not limited to developed countries. As discussed below, recent data indicate that the impact of this disease is increasing in non-Western countries.
The present narrative review of the epidemiology of CHD discusses data on the trends in the prevalence (number of existing cases in a population) and incidence (number of new cases during a specific time) of CHD, with both values used as epidemiological measures of the impact of a disease on a population. Also presented is the information believed to be most relevant to trends in CHD prognosis.
Most information on coronary morbidity and mortality is drawn from data provided by national surveys and observational cohort studies. Although these types of studies are useful, they should be interpreted with caution because they are uncontrolled, with no verification of the accuracy of participant-reported information. Generalization of findings to other periods different from that of the study can also be dangerous and comparisons among studies should be critically interpreted due to possible methodological differences. In this regard, the universal definition of myocardial infarction4 has presented a challenge to the interpretation of measures of the impact of CHD before and after the adoption of the definition in 2000.
Finally, there is considerable variability between studies and official statistics in the terminology, definitions, and condition selected when assessing the impact of CHD in a population. Whereas some statistics refer generically to “ischemic heart disease”, others concentrate on acute myocardial infarction or on acute coronary syndrome (ACS) with or without ST-segment elevation. The following discussion primarily addresses the epidemiology of CHD in general and, where indicated, details specific cases of acute myocardial infarction and ACS.
PREVALENCEEstimation of the true prevalence of CHD in the population is complex. This estimation is often performed via population surveys. Recently, the official statistics office of the American Heart Association published information obtained using this methodology. In particular, the survey estimated that about 15.4 million persons older than 20 years in the United States have ischemic heart disease.5 This figure corresponds to an overall prevalence of CHD among those older than 20 years of 6.4% (7.9% in men and 5.1% in women). For myocardial infarction, the prevalence rate was estimated to be 2.9% (4.2% in men and 2.1% in women).
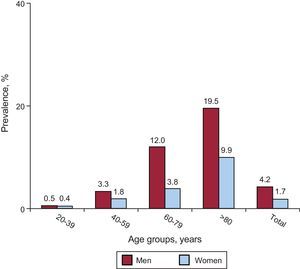
Although the prevalence of CHD increases with age in both men and women, another survey-based American study showed some variation in recent decades in the male:female prevalence ratio in middle-aged persons (35-54 years). Thus, although the prevalence was higher in men than in women in both 1994 to 1998 and 1999 to 2004, this period showed a trend toward a decrease in prevalence in men and an increase in prevalence in women (2.5 vs 0.7 in 1994-1998 and 2.2 vs 1.0 in 1999-2004).6 The most recent data continue to show a strong male predominance in CHD in general and in myocardial infarction in particular in all age groups (Figure 1).5
.")
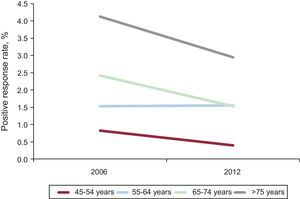
No data are available on the true prevalence of CHD in Spain. Only 1 study from more than a decade ago has directly analyzed the prevalence of angina in the general population, finding rates of 7.3% in men and 7.7% in women.7 However, an indirect approximation can be made via data from the population survey of the Spanish National Institute of Statistics (Instituto Nacional de Estadística). In this survey, participants were periodically asked about “chronic or long-term diseases experienced in the last 12 months”. In the last 2 surveys, explicit reference was made to myocardial infarction, and levels much lower than those of the American population8 were estimated for each age group (Figure 2). Although this survey is obviously vulnerable to the usual biases, because the methodology is similar to that used in other countries, it is not necessary a priori to discard the data when making comparisons with other regions. Moreover, although prevalence is only an indirect approximation, it is valid when analyzing the time course. Thus, a marked decrease can be seen in all age groups in the rate of positive responses to the question on myocardial infarction from the 2006 to the 2012 surveys (Figure 3).
.")

To correctly interpret the above findings, it is necessary to bear in mind that the data obtained from population surveys could underestimate the true prevalence of ischemic heart disease. This underestimation is because ischemic heart disease is often clinically silent or causes few symptoms, even in advanced stages of coronary disease, with silent ischemia estimated to occur in up to 75% of all ischemic episodes.9
INCIDENCEThe incidence rate, defined as the number of new cases of a disease in a specific population and time period, is usually estimated via cohort studies, specific registries, or official statistics, such as discharge record data. Perhaps the study that has provided the most information on the natural history of CHD and, accordingly, its incidence is the Framingham Study. Data from the 44 years of follow-up of the original Framingham Study cohort and the 20 years of follow-up of the offspring of the original cohort have yielded various demographic observations,10–12 particularly the influence of sex and age on the incidence of CHD, which can conceptually be extrapolated to the majority of the population and to the current period.
For example, it is known from the Framingham cohort that the incidence of coronary events rapidly increases with age and that women have rates that are similar to those of men 10 years younger (a mean “delay” of 10 years in the incidence rates). In the case of myocardial infarction and sudden death, the delay in the incidence rates in women is about 20 years, although the margin decreases at older ages.1 The overall incidence of CHD at between 65 and 95 years of age is double for men and triple for women with respect to the rates of those between 35 and 64 years. In premenopausal women, the most critical symptoms of CHD, such as myocardial infarction and sudden death, are relatively rare. Following menopause, the incidence and severity of CHD rapidly increases, reaching rates 3 times greater in postmenopausal women than in premenopausal women of the same age.11
Another general relationship is that, in individuals younger than 65 years, the annual incidence of coronary events in men is higher than the rate of all other atherosclerotic events combined, while in women the rate of coronary events equals the rate of all other atherosclerotic events combined. For those older than 65 years, the incidence of CHD continues to be higher than that of all events secondary to atherosclerosis.
The male predominance in the incidence of ischemic heart disease is lower in the case of angina. Initially, CHD in women younger than 75 years more frequently presents as angina than as myocardial infarction.10 Characteristically, angina tends to be uncomplicated in 80% of these patients, unlike in men, in whom angina appears after a myocardial infarction in 66%. Myocardial infarction predominates among men in all age groups, and only 20% of cases are preceded by angina; this percentage is lower in the case of silent infarction.10,12
Finally, other factors besides sex and age can influence whether ischemic heart disease initially presents as unstable angina or ACS, such as treatment with beta-blockers or statins.13
The Temporal TrendIn general, the incidence of CHD has decreased in recent decades in the United States by between 114 and 133 cases for every 100 000 person-years of follow-up. This reduction has been even higher for cardiovascular disease in general (from 294 to 225 cases for every 100 000 person-years).14 Nonetheless, it is estimated that during 2013 1 citizen of the United States will have a myocardial infarction every 44s.5
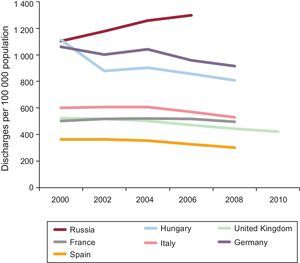
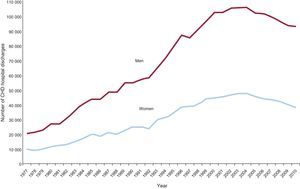
This temporal trend also largely applies to other developed countries but not to developing countries. Data obtained from official statistics of the European Union on cardiovascular disease are shown in Figure 4.3 Regarding the trends for the last decade of high rates of CHD in various European countries, and apart from the well-known differences among countries, a general tendency is seen toward a slight decrease in incidence from mid-way through the previous decade. In Spain, a similar conclusion can be drawn from raw data of the National Institute of Statistics (Figure 5).15 Nevertheless, ischemic heart disease continues to be the main cause of adult death, in both developing and developed countries.16


Number of coronary heart disease hospital discharges by sex in Spain between 1977 and 2010. Reproduced with the permission of Dégano et al.15 CHD, coronary heart disease.
The most marked increases in the incidence of coronary events in the world have been in the Middle East, Latin America, and, to a lesser extent, the Far East. However, there are some differences among regions.17–19 Thus, while the high incidence of ischemic heart disease in India is not explained by traditional risk factors, the tendency in China parallels the trends in these risk factors. For example, in Beijing a considerable increase in the incidence of ischemic heart disease mirrors the unprecedented rise in cholesterol concentrations (from 166 mg/dL in 1968 to 206mg/dL 15 years later). Finally, in Latin America, the trend in the incidence of ischemic heart disease and stroke has largely been exacerbated by increased sedentary behavior, obesity, and smoking.
Myocardial Infarction and Acute Coronary SyndromeAlthough most studies have shown a downward trend in the incidence of myocardial infarction in the United States since the 1970s, some studies have shown contradictory results, above all those that cover the period after 2000,20,21 when physicians began to use troponin as a marker of myocardial necrosis. This method is much more sensitive than the MB fraction of creatine kinase (CK-MB) technique, which could mask a reduction in the infarction rate. In general, the age-adjusted rate of hospitalization due to myocardial infarction was 215/100 000 individuals between 1979 and 1981, which increased to 342 between 1985 and 1987, stabilized in the following decade, and began to decline from 1996 onward, reaching 242 in the 2003 to 2005 period and maintaining a male:female ratio of 2:1,5 but with the same temporal trend in both sexes.
When the estimation refers to ACS, a relative increase has been documented in the incidence of non–ST-elevation ACS (NSTEACS) compared with ST-elevation ACS (STEACS). In the United States National Registry of Myocardial Infarction, the proportion of NSTEACS increased from 19% in 1994 to 59% in 2006. This change in the relative proportion of NSTEACS has been attributed to a decrease in the absolute incidence of STEACS, together with an increase or stabilization in the rate of NSTEACS, depending on whether troponin or CK-MB was used as the diagnostic criterion.5,21 There are, however, some differences between the registries. Whereas 38% of patients in the GRACE (Global Registry of Acute Coronary Events) registry had STEACS, the rate reached 47% in the second EuroHeart Survey.22
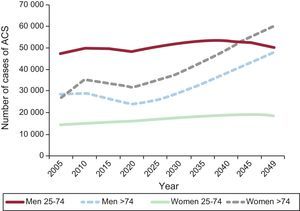
In Spain, a recent methodical analysis of previously published records and official population statistics estimated the following expected distribution of ACS in 2013: 38.2% STEACS, 55.8% NSTEACS, and 6% unclassified ACS.15 This study also calculated a marked expected increase in the incidence of ACS during the next 35 to 40 years, paralleling population aging. Thus, from 2013 to 2049, the number of ACS cases is expected to increase between 69% and 116% in the most advanced age group, with an increased incidence also expected in younger age groups (Figure 6).15

Estimation of the number of expected acute coronary syndrome cases from 2005 to 2049 by sex and age group in the Spanish population. Reproduced with the permission of Dégano et al.15 ACS, acute coronary syndrome.
Ischemic heart disease is the main cause of death in adults in the United States, causing one third of all deaths in individuals older than 35 years.1 The mortality rate is higher in men than in women: 3 times higher in the 25 to 34 age group and 1.6 times higher in the 75 to 84 age group. In the specific case of NSTEACS, various studies have analyzed prognosis in men and women. Although women are associated with a greater presence of comorbidities, they have a similar or even better prognosis than men.23 Regarding racial differences, mortality from ischemic heart disease is higher in blacks than in whites, although these differences disappear at around 75 years. In the Hispanic population, the coronary mortality rate is not as high as that in the black and white populations.
The mortality rates from cardiovascular disease in general and from ischemic heart disease in particular, in men and women as well as in blacks and whites, have fallen between 24% and 50% in developed countries since 1975, although the decrease has been slower since 1990.1,14 In the United States, mortality from cardiovascular disease decreased by 29% from 1996 to 2006. This trend has been observed in both the general incidence of ischemic heart disease and in fatal events, including sudden death and nonsudden cardiac death.24 Approximately 50% of the magnitude of the decrease can be attributed to treatment improvements, both in secondary prevention measures after a coronary event and in the management of the acute phase of ACS, treatment for heart failure, and revascularization for chronic angina. The remaining 50% has been attributed to better risk factor control in the general population, such as reductions in total cholesterol (24%), systolic blood pressure (20%), smoking (12%), and sedentariness (5%).25 These improvements in the control of risk factors in developed countries have been diminished to a certain extent by increases in the mean body mass index and the prevalence of diabetes mellitus, which together are considered to cause about 18% of CHD mortality.
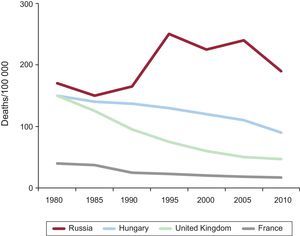
In the United States, the overall reductions in mortality from ischemic heart disease from the 1970s has been 63% in men (from 331 to 121/100 000) and 60% in women (from 166 to 67/100 000).5 In the European Union, mortality from ischemic heart disease has decreased by 32% in men (from 146 to 100/100 000) and by 30% in women (from 64 to 45/100 000). In Eastern Europe, there has been greater variability: mortality from ischemic heart disease increased at the start of the 1990s in some countries and markedly decreased thereafter (Poland and the Czech Republic). The highest mortality rate from ischemic heart disease was found in Russia (330 and 154/100 000 in men and women, respectively, from 1995 to 1998). Overall, the rate of mortality from ischemic heart disease is higher in central and eastern European countries than in the north, south, and west of Europe (Figure 7).3

Regarding other regions, mortality from ischemic heart disease in Japan has traditionally been much lower than in the United States and Europe, with reductions of 29% in men (from 50 to 36/100 000) and of 36% in women (from 28 to 18/100 000). In contrast, mortality from ischemic heart disease is expected to increase in developing countries (China, India, sub-Saharan Africa, Latin America, and the Far East), from an estimated 9 million in 1990 to an expected 19 million in 2020.26,27 The causes of this potential increase are social and economic changes, increased life expectancy, sedentariness, smoking, and a “westernization” of diet.17
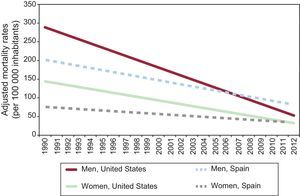
In Spain, recent estimates of the trends in the rate of mortality from myocardial infarction have been compared with those of the United States; a more pronounced relative decrease has been seen in the mortality rate in the United States,28 so that depending on the model, the expected rate of mortality would be lower in the United States than in Spain from 2008 in men and 2012 in women (Figure 8). Nonetheless, application of the same model used in other countries has shown an age-adjusted decrease of 40% in mortality from CHD in Spain from 1988 to 2005.29 It is estimated that 47% of this decrease can be attributed to treatment, mainly that of ACS (11%), and secondary prevention (10%). Accordingly, in parallel with the change in the STEACS:NSTEACS ratio, a significant change has occurred in the treatment of these syndromes, with a progressive therapeutic approach that is more intensive and more in line with the recommendations of scientific bodies, which has considerably decreased in-hospital mortality and associated complications, such as cardiogenic shock and reinfarction.22
 and estimated (2007) rates of mortality from myocardial infarction in the United States and Spain. Reproduced with the permission of Orozco-Beltrán et al.28")
Observed (1990-2006) and estimated (2007) rates of mortality from myocardial infarction in the United States and Spain. Reproduced with the permission of Orozco-Beltrán et al.28
Finally, in the interpretation of these results, it should be remembered that the universal definition of ACS has affected not only the estimation of incidence, but also the estimation of mortality. Thus, in a recent study performed in a coronary care unit, the universal definition of myocardial infarction was associated with an increase both in the diagnosis of infarction (from 55.8% to 70.1%) and the risk of death at 10 years (hazard ratio=1.58; 95% confidence interval, 1.07-2.40; P=.03).
CONCLUSIONSAlthough the incidence of CHD continues to decrease in developed countries, immigration and progressive population aging suggest that the absolute number of coronary events and, consequently, the prevalence of CHD will not decrease and may even increase in the near future. Meanwhile, the globalization of the Western diet and increased sedentary behavior will robustly influence the progressive increase in the incidence of CHD in developing countries, although these counties show considerable variability. While the rate of mortality from CHD has been decreasing in the last 4 decades in Europe, CHD still causes the majority of deaths in certain age groups. Nevertheless, mortality from CHD has progressively decreased, which may be due to both treatments for the acute phase of ACS and preventive measures.
CONFLICT OF INTERESTSNone declared.
Sección patrocinada por AstraZeneca