Childhood obesity trends are plateauing in Spain, but limited information is available about how they differ by region. This study assessed childhood and adolescent the prevalence and incidence of overweight and obesity from 2005 to 2017 across 8 Spanish regions.
MethodsThis longitudinal study used height and weight measurements from 2.5 million children aged 2 to 17 years to calculate overweight and obesity, according to the World Health Organization (WHO) guidelines. Data were obtained from The Base de datos para la Investigación Farmacoepidemiológica en Atención Primaria, and the Information System for Research in Primary Care. Prevalence and incidence rates and trends from 2005 to 2017 were calculated and stratified by age, sex, and region.
ResultsThe overall obesity prevalence increased in boys and girls from age 2 (0.8%; 95%CI, 0.8-0.9 in both sexes) until peaking at age 7 in girls (17.3%; 95%CI, 17.1-17.5) and age 9 in boys (24.1%; 95%CI 23.9-24.3). The highest and lowest obesity prevalences were observed in Murcia and Navarre. Overall obesity prevalence trends decreased from 2005 to 2017 in all age-sex groups and in most regions. Highest obesity incidence rates were found in children aged 6 to 7 years, (4.5 [4.5-4.5] and 3.5 [3.5-3.5] new obesity cases per 100 person-years in boys and girls, respectively). Boys had higher prevalence and incidence rates than girls across all regions. Overweight/obesity prevalence and incidence rates and their trends were consistently higher than the obesity results, although a similar pattern was observed across sex and age.
ConclusionsOverweight and obesity prevalence slightly decreased in Spain from 2005 to 2017, but regional, sex, and age differences persisted. Because incidence peaked around the age of 6 years, it may be important to begin health promotion programs at an early age.
Keywords
Excess weight among children and adolescents is currently a major public health concern due to its high global prevalence and associated risk of negative health outcomes, including cardiovascular, musculoskeletal, and endocrine diseases.1–3 Current literature suggests that childhood obesity prevalence has plateaued or is slightly decreasing in most developed countries, including Spain.4–6 Despite this, Spain continues to have the second highest childhood overweight and obesity prevalence in Europe.7 However, overweight and obesity prevalence is not homogenous across all of Spain, but rather differs by region.8 Typically, higher prevalences are found in the southernmost regions of the country.8,9
Previous studies in Spain have been mainly cross-sectional,10,11 relied on self-reported national health survey data,6,8 or included data on only one or few regions.9,12–14 Few studies have used longitudinal data to calculate prevalence trends and incidence rates across multiple regions.
Trend analysis studies are an important tool for monitoring changes and patterns in the prevalence and incidence of overweight and obesity.15 Knowledge of these trends can be used to plan public health interventions directed toward regions or population subgroups whose trends are worsening or not reversing. Because they provide longitudinal data on large populations, electronic health records are useful for population health surveillance. Within the past few decades, electronic health records have been successfully used to assess childhood and adolescent overweight and obesity trends.14,16 Despite their utility, few studies have used data from electronic health records to assess incidence trends of overweight and obesity among children and adolescents.14,17 The aim of this study was to examine the prevalence and incidence of overweight and obesity and their trends between the years 2005 and 2017 among 2.5 million children and adolescents between the ages of 2 and 17 years across 8 Spanish regions.
METHODSData sourcesWe obtained deidentified data from 2 primary care electronic health records databases: the BIFAP (Base de Datos para la Investigación Farmacoepidemiológica en Atención Primaria [Database for Pharmacoepidemiological Research in Primary Care]) and the SIDIAP (Sistema de Información para el desarrollo de la Investigación en Atención Primaria [Information System for Research in Primary Care]). Both rely on data from the regional health services integrated in the Spanish national health system, which provides universal access to health care to the entire Spanish population. Both databases contain demographic data and height and weight measurements recorded at repeated intervals during childhood and adolescence by pediatric primary care health professionals. BIFAP is a multiregional dataset that, in 2017, contained data for 9.4 million people from 7 out of the 17 autonomous regions of Spain, starting in 2001.18 The data are provided by primary care health professionals on a voluntary basis in some regions and include the entire population in others. At the time of the study, BIFAP included data from of 6857 primary care physicians (5862 general practitioners and 995 pediatricians) from 7 regions (Aragon, Asturias, Cantabria, Castile and Leon, Madrid, Murcia, and Navarre). This yields a total of 9.4 million patients, representing 67% of the population of these regions (14 million) and 20% of the total Spanish population (46.5 million). The population of BIFAP is representative of the population receiving health care in the Spanish national health system,18 which covers nearly the entire population (99.02% in 2017). For its part, SIDIAP contains data on nearly 6 million people from 286 primary care health centers in the region of Catalonia starting in 2005.19 The population of SIDIAP is highly representative of Catalonia in terms of geographical, age, and sex distributions.20
Study population and study designIn this prospectively-collected longitudinal study, we included all children and adolescents registered in BIFAP and SIDIAP between the ages of 2 and 17 years with at least 1 height and weight measurement recorded during the same primary care visit from 1 January 2005 to 31 December 2017 (or from 1 January 2011 for Castile and Leon).
Anthropometric measuresHeight and weight were routinely measured in a standardized fashion by trained pediatric primary care health professionals as part of the health promotion program “Programa de Salud Infantil” (Childhood Health Program).21 The program recommends measuring height and weight at several key points during childhood and adolescence: at 2 years, 3 to 4 years, 6 to 7 years, 8 to 9 years, 12 years, and 14 years.21 Body mass index (BMI) was calculated as weight (in kilograms, kg) divided by height (in meters, m) squared. Overweight and obesity were defined using the age- and sex-specific BMI z-scores (zBMI) from the World Health Organization (WHO) growth standard and growth reference.22,23 Overweight was defined as a zBMI greater than+2.0 in children younger than 5 years or greater than+1.0 in those older than 5 years. Obesity was defined as a zBMI greater than+3.0 in children younger than 5 years or greater than+2.0 in those older than 5 years. Extreme values of height, weight and BMI (zBMI>±5.0) were removed.24 If a child had more than 1 BMI measurement for the same age or study year, we considered the most recent available BMI measurement. Biologically-implausible values of height and weight were removed.24,25
Statistical analysesWe calculated overweight and obesity prevalence and 95% confidence intervals (95%CI) as the percentage of children with overweight (including obesity, denoted by overweight/obesity) or obesity from the entire study population, stratified by age, sex, study year, and region. We grouped age into 3 categories (2-5 years, 6-11 years, and 12-17 years) to evaluate prevalence trends. We calculated P-trends using a logistic regression model with study year as a continuous variable and overweight/obesity and obesity (vs nonoverweight/obesity or no obesity) as a binary variable. Next, we calculated the percent change of prevalence between the years 2005 to 2017 by dividing the difference of the prevalence in 2005 and 2017 by the prevalence in 2005 and multiplying by 100.
For all children with at least 2 recorded BMI measurements, we calculated overweight/obesity incidence rates (for children with normal weight at baseline) and obesity incidence rates (for children with normal or overweight at baseline). Children were followed up until they developed overweight/obesity (if they were of normal weight at baseline), obesity (if they were of normal weight or overweight at baseline), turning 18 years old, reaching the end of the study (31 December 2017), death, or being transferred out. Incidence rates were calculated by dividing the number of new cases of overweight or obesity by 100 person-years. Person-years are the time (in years) that a child is at risk of developing overweight/obesity or obesity during a specific age period. Because the number of observations was higher in even-numbered ages (especially at ages 4, 6, 8, 12, and 14 years), age periods were grouped into 2 consecutive years (2-3, 4-5, 6-7, 8-9, 10-11, 12-13, 14-15, and 16-17 years). To observe incidence trends, we estimated the incidence rates during 2 time periods: from 1 January 2006 to 30 June 2011 and from 1 July 2011 to 31 December 2017.
Our presentation of the results focuses primarily on the prevalence and incidence of obesity, with the results of overweight/obesity provided in the . All the above analyses were conducted in R.26 This study was approved by the scientific committee of BIFAP (code: 06_2018) and the Ethics committee of IDIAPJGol (code: P16/179).
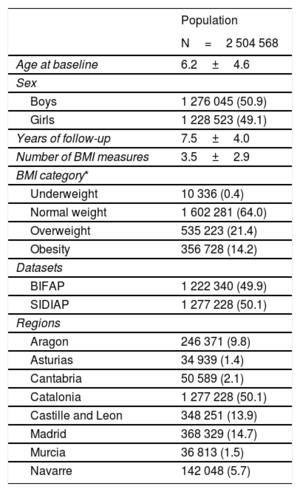
RESULTSStudy population descriptionThe study populations included 2504568 children with 7613323 BMI measurements from 8 Spanish regions. A total of 1278045 children (51% of the study population) were boys. Overall, the study population had an average baseline age of 6.2 years (standard deviation [SD] 4.6), were followed up for an average of 7.5 (SD, 4.0) years and had an average of 3.5 BMI (SD, 2.9) measurements during follow-up (table 1); 35.6% and 14.2% of the children had at least 1 measurement indicating overweight/obesity and obesity during follow-up, respectively (table 1). Children living in Catalonia had the longest average follow-up time (8.8 years; SD, 3.9) whereas children living in Castile and Leon had the shortest follow-up time (4.8 years; SD, 2.0). The population from Navarre and Catalonia had the highest and lowest average number of BMI measurements, respectively (Navarre, 9.0 vs Catalonia, 3.9 BMI measures per child) ().
Characteristics of children and adolescents (2-17 years) included in the study from 2005 to 2017
| Population | |
|---|---|
| N=2 504 568 | |
| Age at baseline | 6.2±4.6 |
| Sex | |
| Boys | 1 276 045 (50.9) |
| Girls | 1 228 523 (49.1) |
| Years of follow-up | 7.5±4.0 |
| Number of BMI measures | 3.5±2.9 |
| BMI category* | |
| Underweight | 10 336 (0.4) |
| Normal weight | 1 602 281 (64.0) |
| Overweight | 535 223 (21.4) |
| Obesity | 356 728 (14.2) |
| Datasets | |
| BIFAP | 1 222 340 (49.9) |
| SIDIAP | 1 277 228 (50.1) |
| Regions | |
| Aragon | 246 371 (9.8) |
| Asturias | 34 939 (1.4) |
| Cantabria | 50 589 (2.1) |
| Catalonia | 1 277 228 (50.1) |
| Castille and Leon | 348 251 (13.9) |
| Madrid | 368 329 (14.7) |
| Murcia | 36 813 (1.5) |
| Navarre | 142 048 (5.7) |
BIFAP, Base de Datos para la Investigación Farmacoepidemiológica en Atención Primaria (Database for Pharmacoepidemiological Research in Primary Care); BMI, body mass index; SIDIAP, the Information System for Research in Primary Care.
Values are expressed as No. (%) or mean±standard deviation.
Children were categorized as obese if they had at least 1 zBMI classified as indicating obesity during the study period. Children were categorized as being overweight/obese f they had at least 1 zBMI classified as indicating overweight or any measurement classified as indicating obesity during the study period. Finally, children were categorized as having normal weight if they were never categorized as being overweight or obese during the study period.
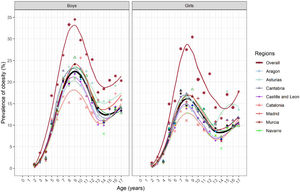
The overall prevalence of obesity increased in boys and girls, starting at age 2 years (0.8%; 95%CI, 0.8-0.9 in both sexes) until peaking at age 7 years in girls (17.3%; 95%CI, 17.1-17.5) and age 9 years in boys (24.1%; 95%CI, 23.9-24.3), before decreasing until age 14 years ( and figure 1). After age 14 years, there was a slight increase until age 17 years in both sexes (from 10.6%; 95%CI, 10.5-10.7 at age 14 years to 13.4%; 95%CI, 13.0-13.7 at age 17 years in boys, and from 6.7%; 95%CI, 6.6-6.8 at age 14 years to 10.2%; 95%CI, 10.0-10.5 at age 17 years in girls) (figure 1 and ). The prevalence of overweight/obesity followed roughly this same trend. The prevalence of overweight/obesity peaked in both sexes at age 9 years (46.6%; 95%CI, 46.6-46.9 in boys and 43.7%; 95%CI, 43.5-44.0 in girls) before decreasing until age 14 years ().

Prevalence of obesity by sex and age in 2 504 568 children in the overall population and by region. Each dot represents the prevalence of obesity for each child age and applied a weighted loss smoother to observe the trends over time. The last measurement was used for the same age year if a child had more than one BMI measurement.
All regions followed a similar pattern to the overall prevalence of obesity (figure 1 and ). The highest obesity prevalence was observed in Murcia at age 9 years, especially in boys (34.5%; 95%CI, 30.6-38.4) compared with girls (30.4%; 95%CI, 26.9-33.9). The lowest prevalence was observed in Navarre at age 9 years (21.0%; 95%CI, 20.0-21.9 in boys and 14.2%; 95%CI, 13.4-14.9 in girls) (). In Asturias, Cantabria, Catalonia, and Madrid, the prevalence of obesity was slightly higher than the overall prevalence of obesity, whereas in Aragon and Castile and Leon the prevalence was similar to the overall prevalence of obesity (figure 1 and ). The highest prevalence of overweight/obesity was also found in Murcia and the lowest prevalence in Navarre ().
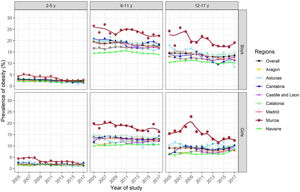
Overweight and obesity prevalence trendsOverall obesity trends decreased in all age-sex groups from 2005 to 2017 (figure 2 and ). In boys ages 6-11 years, the overall prevalence of obesity decreased from 19.5% (95%CI, 9.2-19.8) in 2005 to 17.6% (95%CI, 17.4-17.8) in 2017 (figure 2 and ), corresponding to a 9.7% change (figure 3 and ). Although the prevalence was low compared with that in other age groups, the largest decreases were generally found in ages 2 to 5 years. For example, for boys, the overall trend at ages 2 to 5 years fell from 3.0% (95%CI, 2.9-3.1) in 2005 to 2.1% (95%CI, 2.0-2.2) in 2017 (figure 2 and ). These changes corresponded to a 30.0% decrease (). The overall prevalence of overweight/obesity followed a similar decreasing trend (). For example, in boys aged 6 to 11 years, the overall prevalence of overweight/obesity decreased from 42.2% (95%CI, 41.8-42.5) in 2005 to 37.8% (95%CI, 37.5-38.1) in 2017, corresponding to a 10.4% change ().
, and region. Each dot represents the prevalence of obesity for each child age and applied a weighted loss smoother to observe the trends overtime. The last measurement was used for the same age year if a child had more than one BMI measurement.")
Prevalence trends of obesity between 2005 and 2017 by sex, age groups (2-5 years, 6-11 years, 12-17 years), and region. Each dot represents the prevalence of obesity for each child age and applied a weighted loss smoother to observe the trends overtime. The last measurement was used for the same age year if a child had more than one BMI measurement.

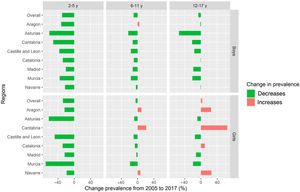
Percent change in the prevalence of obesity between 2005 and 2017 by age, sex, and region. The percent change of prevalence from 2005 to 2017 was calculated by dividing the difference between the prevalence in 2005 and 2017 by the prevalence in 2005 and multiplying by 100. For Castille and Leon the difference was calculated between 2010 and 2017.
The prevalence of obesity decreased over time in nearly all regions, especially among children aged 2 to 5 years (figure 2). However, slight differences were observed especially for girls aged 6 to 11 years and 12 to 17 years in Aragon, Cantabria and Navarre where the prevalence fell only gradually, or even increased (figure 2 and ). For example, for girls aged 12 to 17 years in Navarre, prevalence increased from 6.6% (95%CI, 5.7-7.4) in 2005 to 8.3% (95%CI, 7.4-9.2) in 2017 (figure 2 and ). Prevalence decreased in most other regions, particularly in Murcia for girls aged 12 to 17 years, where the prevalence decreased from 15.4% (95%CI, 10.8-20.0) in 2005 to 12.4% (95%CI, 9.9-14.9) in 2017. The overweight/obesity trends decreased in all regions and in both sexes among children aged 2 to 5 and 6 to 11 (). Similar to the prevalence of obesity, that of overweight/obesity in girls decreased more gradually than in boys and increased in Aragon, Catalonia and Navarre in ages 12-17 years ().
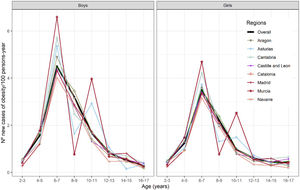
Incidence of overweight and obesityThe overall incidence rate of overweight and obesity peaked between the ages of 6 to 7 years in both sexes (figure 3 and ). After this peak, the incidence rates continued to decrease into adolescence. The number of new obesity cases per 100 person-years was 4.5 (95%CI, 4.5-4.5) in boys and 3.5 (95%CI, 3.5-3.5) in girls aged 6 to 7 years (figure 3 and ). Obesity incidence rates were highest in Murcia for both sexes (6.6; 95%CI, 6.1-7.1 in boys and 4.7; 95%CI, 4.3-5.1 in girls aged 6 to 7 years) and were lowest in Navarre (4.0; 95%CI, 3.9-4.2 in boys aged 6 to 7 years and 3.2; 95%CI, 3.0-3.3 in girls aged 6 to 7 years) (figure 3 and ). The incidence rates by region followed a similar pattern as the overall incidence, except for Asturias and Murcia where we observed low incidence rates in both sexes in ages 8 to 9 years (1.6; 95%CI, 1.4-1.9 and 0.8; 95%CI, 0.6-1.0 in boys living in Asturias and Murcia, respectively) and high incidence rates between ages 10 and 11 years (2.9; 95%CI, 2.6-3.3 and 4.0; 95%CI, 3.5-4.4 in boys living in Asturias and Murcia, respectively). Overweight/obesity incidence rates followed roughly the same trend as obesity for age, sex, and region (). Additionally, we observed that the overall incidence of overweight/obesity and obesity decreased from the first to the second period in all age groups and both sexes (). We could not calculate incidence trends by region due to the small sample size and confidentiality issues (figure 4).
DISCUSSION of obesity by sex, age and region.")
To our knowledge, our study is the largest to date to evaluate the prevalence and incidence of overweight and obesity rates in children and adolescents across 8 Spanish regions. A higher prevalence of overweight and obesity was found in children aged 9 years and was consistently higher among boys and in the southern region of Murcia. Overweight/obesity and obesity prevalence and incidence trends slightly decreased between 2005 and 2017 across age, sex, and region. However, in Aragon, Cantabria and Navarre, overweight/obesity and obesity prevalence trends remained constant over time, and even increased in girls older than 6 years. Incidence rates were highest at ages 6 to 7 across all regions and both sexes, but were higher in boys than in girls and in southern regions than in northern regions. Previous studies found similar results with higher incidence rates around middle childhood (6-11 years), decreasing into older ages.17 The decrease in incidence could be explained by fewer children being are at risk of developing overweight and obesity, or by several development changes occurring during puberty such as an adiposity rebound and hormone composition, which may stabilize their weight during adolescence.17
The overall overweight and obesity prevalence by age and sex in our study was lower than in other nationally representative studies4,6 (). The lower prevalence could be explained by the fact that our study did not include data from regions where the highest overweight and obesity prevalence has historically been found, such as Andalusia and the Canary Islands.27 Additionally, the prevalence of childhood overweight and obesity seems to have stabilized or even decreased in Spain since 2005, as in other high-income countries.1,3,4,6 However, Spain continues to have some of the highest childhood overweight and obesity prevalences in Europe, on average 5% to 10% units higher than in other European countries.7
In Spain, few studies have evaluated the changes in overweight and obesity prevalence in children at the national level. Data from the Spanish National Health Survey found no significant changes in the prevalence of overweight or obesity between 2001 and 2011,6 whereas another nationally representative study found only a very slight reduction in the prevalence of overweight and obesity between 2011 and 2019.4 A comparable study performed only in Catalonia also found a slight decrease in overweight and obesity prevalence during the last decade.14 Having access to a large sample size and repeat height and weight measurements may have helped our study to reveal slight trend differences over the last decade. The specific mechanisms for the stabilization and reduction of childhood obesity remain unclear. It is possible that obesity rates have reached a saturation point or that public health initiatives have successfully raised awareness of the health problems associated with childhood obesity and changed behaviors.1,28
Because the highest incidence rates of overweight and obesity were observed between the ages of 6 and 7 years, it may be important to begin obesity prevention and health promotion programs at an early age.14,17,28 However, only a few interventions aiming to reduce BMI and prevent childhood obesity before the age of 6 years have been identified, suggesting that this may still be a new and developing consideration.29 Current literature suggests that, across all of childhood, individual-level interventions may be slightly more effective than community-based interventions in the short-term.30,31 For example, individual-level interventions carried out among Australian children aged 3 to 6 years32 and American children aged 2 to 5 years33 that aimed to improve nutrition and physical activity levels found significant reductions in zBMI scores. Community-based interventions have not always shown conclusive results of their effectiveness.34 For example, a community-based intervention implemented in Spain among children aged 8 to 10 years did not improve weight development, diet quality, or physical activity levels in the short-term.34 However, an individual-level intervention performed among Spanish children aged 9 to 10 years that aimed to improve diet and increase sleep and physical activity levels while reducing screen time significantly reduced the incidence of childhood obesity.35 The success of this individual-level intervention, although not performed at an early age, suggests that individual-level interventions may be an important starting point to immediately reduce the high childhood overweight and obesity prevalence present in Spain.
The findings of our study suggest that childhood obesity prevalence and incidence rates vary by region in Spain. The most recent data available by region suggests a similar pattern, revealing the highest prevalence trends and incidence rates among the southern region of Murcia and the lowest in Navarre.11 However, no previous study has evaluated both the prevalence trends and incidence rates of overweight and obesity by region with such a large sample using data from primary care electronic health records. Regional differences in overweight and obesity prevalence may mirror the regional socioeconomic disparities in Spain, where less-industrialized regions tend to face higher levels of deprivation and more industrialized regions tend to be less deprived.36 Children living in more deprived areas are known to consume more energy-rich foods, have lower levels of physical activity, and have reduced access to interventions and educational services, all of which increase the risk of developing obesity during childhood.37–41 We have no clear explanation as to why the trends in Cantabria, Aragon and Navarre are increasing, especially among girls older than 6 years. The peak in medical visits between ages 10 and 11 years in Asturias and Murcia may explain the differences in incidence compared with other regions.
Boys consistently have a higher prevalence of obesity than girls across all regions of Spain, suggesting possible differences by sex. In fact, all prevalence studies performed in Spain have shown these same differences by sex.6,8,14,42 Differences in childhood overweight and obesity patterns by sex could be explained by many mechanisms, such as body composition, hormones, differences in physical activity levels, and gendered societal pressure and expectations.11,43–46 Interventions that take into account gender-based differences in physical activity levels, relationship with food, and body image may be useful in reducing these observed disparities.
Strengths and limitationsOne of the main strengths of our study, in addition to its sample size and longitudinal design, is the availability of repeat measurements of weight and height for the same child. Furthermore, we were able to evaluate prevalence trends for 8 Spanish regions using the same study design and only 2 databases. Both of these databases are representative of the Spanish population, allowing our results to be interpreted with high external validity.
However, our study has some limitations. First, we were limited to studying the regions for which data were available through the SIDIAP and BIFAP. Consequently, our results likely underestimate national overweight and obesity prevalence, but are representative of the specific regions of Spain.9,12,13 Next, we only had data available on children who used the public Spanish health care system. Within the public health care system, obesity may be slightly overestimated as children with obesity have more medical visits than healthy children. However, all the regions have implemented the Childhood Health Program (Programa de Salud Infantil), which recommends several medical appointments at key points during childhood to combine preventive and health promotion activities. Due to the standardized timeline of the Childhood Health Program included in the public health care system, and our large sample size, we expect obesity overestimation to be minimal. Finally, we did not have additional information of other sociodemographic factors such as socioeconomic status or nationality, which are known to affect childhood obesity prevalence and incidence differently.14
CONCLUSIONSOverall, overweight and obesity trends have slightly decreased in Spain since 2005 and the highest incidence rates were found in ages 6 to 7 years. Regional and gender disparities persist, with higher prevalence and incidence rates in boys than in girls and in southern than in northern regions. New and innovative approaches that take into account gender-based and regional differences must be used to create public health interventions to reduce excess weight starting from an early age.
- -
Childhood overweight and obesity prevalence seems to have plateaued or slightly decreased in Spain.
- -
However, Spain continues to have the second highest childhood overweight and obesity prevalence in Europe.
- -
To date, few longitudinal studies have been performed on the topic and few studies have analyzed prevalence and trends and incidence across multiple Spanish regions in a single study.
- -
Our study shows that, despite decreasing trends of overweight/obesity and obesity at the national level, differences by gender and region persist.
- -
Higher prevalence and incidence rates were found in southern than in northern regions. Our study also confirms gender-based differences across all regions, with consistently higher prevalence and incidence rates being found in boys than in girls.
- -
Because the highest incidence was found at age 6 years, it may be important to start metabolic health interventions at an early age.
This project was funded by La Marató de TV3 Fundaciò (Grant Number: 201621-30). T. Duarte-Salles is funded by the Department of Health of the Generalitat de Catalunya, awarded on the 2016 call under the Strategic Plan for Research and Innovation in Health (PERIS) 2016-2020, modality incorporation of scientists and technologists, with reference SLT002/16/00308.
AUTHORS’ CONTRIBUTIONST. Duarte-Salles confirms that all authors of this research article have made substantial contributions to the creation and design of the work, have directly participated in the planning and execution of the work, and have approved the final version we are submitting. J. de Bont and M. Bennett share first authorship of this publication.
CONFLICTS OF INTERESTThe authors have no conflict of interest to declare.
Supplementary data associated with this article can be found in the online version available at https://doi.org/10.1016/j.rec.2021.07.002