Keywords
INTRODUCTION
Atrial fibrillation (AF) is the most common arrhythmia. Its prevalence among the general population ranges around 0.95% and increases with age, being 0.1% in individuals under 55 years of age and up to 9% in patients over the age of 80 years.1,2 Although it can be asymptomatic, it is usually associated with a wide variety of symptoms, such as palpitations at rest and/or exertion, dyspnea, chest pain, dizziness, syncope, etc.
Atrial fibrillation is classified, on the basis of the form of clinical onset as paroxysmal, persistent or permanent.1 Treatment is influenced by the dynamic nature of the course of the disease and, thus, it is necessary to review and update the type of AF in each patient.3 Over the past decade, studies have been carried out to compare the effect on survival of different therapeutic strategies in patients with AF, and have shown there to be no significant differences.1 Consequently, improvement of the symptomatology and health-related quality of life (HRQoL) are presently the main objective of treatment for AF.1,3
While AF, as a disease, has been extensively studied, its impact on the HRQoL of affected patients has received less attention. At the present time, different methods for evaluating the impact of AF on the HRQoL of the patients are available, but generic questionnaires such as the SF-36, rather than specific questionnaires, have usually been employed for this purpose.4,5 The studies performed show that the HRQoL is influenced by variables such as age and sex, the New York Heart Association (NYHA) functional class6 and the presence of concomitant diseases.7,8 In contrast, although the HRQoL of all the patients with AF improves over time, there are no statistically significant differences in the HRQoL regardless of the therapeutic strategy employed (rhythm versus rate control).9-11 It is known that, in general, the HRQoL of AF patients is limited and that the majority of the patients subjected to a health intervention experience a clear improvement in their HRQoL.12-14 However, the influence that the different types of AF may have on the HRQoL of the patient has not previously been analyzed.
Thus, we raise the question of the need to carry out an evaluation using a validated specific questionnaire that is capable of detecting differences in the HRQoL of these patients. It was for this purpose that the Atrial Fibrillation-Quality of Life (AFQoL) questionnaire was designed15 and validated.16 With this specific assessment tool, differences could be detected between the three types of AF and the various alternatives for their clinical management, which, at the present time cannot be properly evaluated by means of generic questionnaires.
The purpose of this study was to analyze the possible differences in the HRQoL of the patients, according to the type of AF they had, using the AFQoL specific questionnaire.
METHODS
Study Design
A prospective, observational, multicenter study was carried out under conditions of routine clinical practice in Spain. A total of 29 cardiologists specializing in arrhythmias participated in the study, which was evaluated and approved by the obligatory ethics committees. The results presented here are part of a subanalysis of the validation study of the AF-QoL questionnaire.16
Three study groups were included in the questionnaire validation study: patients with any type of AF who had undergone some type of therapeutic intervention, patients with any type of AF in stable clinical condition, and a control group of patients with myocardial infarction more than 1 year earlier and in stable clinical condition. All of the patients were over 18 years of age. Patients whose diseases could mask the results of the study and those who were included in any kind of clinical trial were excluded.16 For this subanalysis, the data collected were analyzed according to the type of AF.
Although the original study involved 1 follow-up visits on the part of the AF patients, the present subanalysis was carried out considering exclusively the information collected in the baseline visit. The information recorded at that time included sociodemographic data (age and sex), type of AF (paroxysmal, persistent, or permanent), presence of structural heart disease and type, concomitant diseases, number of hospital admissions and visits to the emergency department for cardiac-related causes, echocardiographic findings (left atrial dilatation, left ventricular systolic dysfunction), associated symptoms (palpitations, dizziness/ syncope, dyspnea, chest tightness and other poorly defined symptoms), NYHA functional class, and therapeutic strategy (control of the rate or rhythm) of each patient. Moreover, the patients were given the AF-QoL and SF-36 questionnaires, although, in the present report, only the results obtained with AF-QoL were analyzed.
AF-QoL Questionnaire
The AF-QoL questionnaire15,16 is a specific questionnaire with 18 items, grouped in 3 dimensions, with Likert-type responses with 5 categories. The items in the AF-QoL questionnaire refer to the month preceding the visit, and the score ranges from 0 (poorest HRQoL) to 100 (best HRQoL). The AFQoL questionnaire has been found to be a useful tool in clinical practice, showing proof of its feasibility, validity, and reliability.16
Statistical Analysis
A descriptive and comparative analysis of the sociodemographic and clinical characteristics of the patients was carried out, according to the type of AF, using Student t test or analysis of variance (ANOVA) in the case of the continuous variables (or their nonparametric equivalents, the Mann-Whitney U or Kruskal Wallis test). For the categorical variables, the chi-square test was employed. Student t test was utilized to compare the AF-QoL questionnaire scores among the types of AF. To compare the scores obtained in the AF-QoL questionnaire in terms of the clinical variables, the Mann-Whitney U test, Kruskal-Wallis test, or Spearman's correlation coefficient was used, depending on the variable analyzed. For multiple comparisons, the Scheffé method was employed.
In addition, for the purpose of determining the influence that the characteristics of the patient and of the disease itself could have on the HRQoL, multivariate linear regression analyses were carried out, utilizing, as dependent variables, the different AF-QoL questionnaire scores for each of its dimensions (psychological, physical, sexual, and overall) and, as independent variables, those that had exhibited a level of significance of P<.05 in the bivariate analysis performed previously (age, sex, time elapsed since detection of AF, concomitant diseases, left atrial dilatation, left ventricular systolic dysfunction, structural heart disease, number of visits to the emergency department for cardiac-related causes within the preceding year, NYHA functional class, and type of AF). Both the frequency and the duration of the symptoms are variables that are closely correlated with the type of AF and, thus, were not included to avoid problems of colinearity in the model.
The analysis was performed with the SPSS 15.0.1 statistical software package for Windows, and the differences between the types of AF were considered to be statistically significant at a P value <.05.
RESULTS
In total, 341 patients with AF were included in the study; 42.9% had persistent AF (n=144), 37.5% had paroxysmal AF (n=126), and 19.6% had permanent AF (n=66).
Table 1 summarizes the major sociodemographic and clinical characteristics of the patients. Statistically significant differences depending on the type of AF were observed in all the variables analyzed, with the exception of sex and number of hospital admissions over the preceding year. In the group of patients with permanent AF, the mean age, time elapsed since the diagnosis of AF, size of left atrium, and incidence of structural heart disease were significantly greater than those of the groups of patients with persistent or paroxysmal AF. Moreover, they also had a greater rate of comorbidity (83.3% of the patients had some associated disease, mainly hypertension and/or dyslipidemia) and a higher mean number of diseases per patient (1.48; standard deviation [SD]: 1.01).

With respect to hospital admissions over the preceding year (Table 1), no significant differences were found between the groups of patients (P=.85). However, when the number of visits to the emergency department due to cardiac-related causes during the same period of time was considered, a significant increase was observed in the percentage of patients with paroxysmal AF that required this type of service with respect to the rest of the patients included. Those with paroxysmal AF required an average of 2.2 (SD=1.7) visits to the emergency room, whereas the average number of visits on the part of the patients with persistent or permanent AF was less than 2 (P<.05).
Most of the patients with paroxysmal AF were in NYHA functional class I, whereas the majority of the patients with permanent and persistent AF were in functional class II.
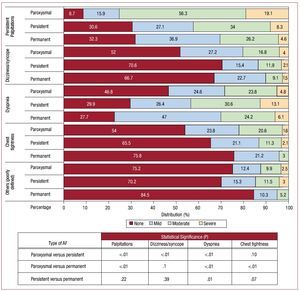
The patients in the paroxysmal AF group exhibited a higher incidence of associated symptomatology than the patients with persistent or permanent AF, mainly palpitations and chest tightness (Figure 1). In contrast, a higher percentage of patients with persistent AF and, above all, permanent AF, had dyspnea. Moreover, the mean number of symptoms was 4.5 (SD=2.5) in the patients with paroxysmal AF, 3.8 (SD=2.4) in persistent AF and 3.1 (SD=2) in permanent AF (P<.05).

Figure 1. Distribution of patients with atrial fibrillation (AF) according to the associated symptomatology and type of AF.
The therapeutic strategy differed depending on the type of AF: 75.4% of the patients with paroxysmal AF and 59% of the patients with persistent AF received treatment to control the cardiac rhythm, whereas in the case of the patients with permanent AF, the most widely used treatment was aimed at controlling the rate (77.3%). A minority of the patients received no specific treatment for AF (4% of the patients with paroxysmal AF, 7.6% of those with persistent AF and 3% of those with permanent AF).
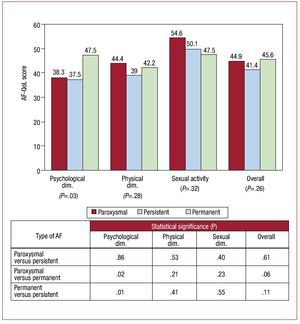
There were no differences in the total score or in the physical or sexual dimensions of the AF-QoL according to the type of AF (Figure 2). However, in the psychological dimension, the patients with permanent AF had a better HRQoL (47.5 points) than the patients with paroxysmal AF (38.3 points; P=.02) or persistent AF (37.5 points; P=.01). The multivariate analysis, the results of the tests for significance of which are shown in Table 2, demonstrated that the differences observed in the psychological dimension of the AF-QoL would be attributable to the type of AF, since statistical significance was not observed in any of the other variables considered. The analysis also showed that the number of visits to the emergency department during the preceding year and the functional class could cause an interaction with the HRQoL in these patients (P<.05).

Figure 2. Mean scores obtained in the Atrial Fibrillation-Quality of Life (AF-QoL) questionnaire by patients with atrial fibrillation (AF); dim.: dimension.

The occurrence of symptomatic episodes in a patient, in any of the types of AF, was associated with a decrease in the HRQoL score (poorer HRQoL) of that patient. Moreover, the frequency of the development of the symptoms of AF also had a negative impact on the HRQoL in these patients. The higher the frequency of the symptoms of AF, the lower the score obtained in the AF-QoL questionnaire.
With regard to the number of visits to the emergency department for cardiac-related causes over the preceding year, a correlation was observed between the number of visits and a decrease in the HRQoL in the case of the patients with paroxysmal AF (r=-0.19; P=.04) and persistent AF (r=-0.40; P<.01).
Patients with a better functional capacity (according to the NYHA) also had a better HRQoL.
Finally, with respect to the AF-QoL score according to the therapeutic strategy utilized (control of rate, control of rhythm or absence of treatment), no statistically significant differences were observed in the HRQoL in any type of AF.
DISCUSSION
The use of the specific AF-QoL questionnaire has made it possible to demonstrate that the HRQoL of AF patients does not differ according to the type of AF. Differences in the AF-QoL score have only been observed in the psychological dimension of the questionnaire, with those patients with permanent AF exhibiting a better HRQoL in this dimension. These differences could be attributable to the important psychological factor associated with the mode in which the course of the disease develops. In this respect, it has been observed that a third of the patients with AF have high levels of depression and anxiety.12
It should be pointed out that most of the patients included belonged to the persistent and paroxysmal AF groups, with less than 20% of the entire group having permanent AF. This fact could constitute a limitation to the study since the sample size for an analysis according to the type of AF was not previously calculated (the previous stratification of the sample according to types of AF was not performed), and the recruitment was maintained according to routine clinical practice. The small number of patients with permanent AF included could be due to the fact that fewer of these patients, who are clinically stable, are referred to arrhythmia specialists, as well as to their more advanced age (which could make them poorer candidates for the administration of the questionnaire) and to the disease prognosis itself. The sample included was calculated to ensure the objectives of the main study (validation of the AF-QoL),16 and not for this subanalysis.
The patients with permanent AF, in addition to being those with the oldest mean age, were those in whom a longer time had elapsed since diagnosis (6.8 years) and, thus, a longer disease course and probably a greater adaptation to the condition. The patients in whom the disease is permanent may have the perception that the symptoms become milder or even disappear, especially in those of advanced age.17 In this respect, the scores obtained in the psychological dimension of the AF-QoL questionnaire would indicate that it is precisely the patients with permanent AF who experience a better HRQoL in this aspect due to their better adaptation to the disease.18
The administration of the AF-QoL questionnaire and the multivariate analysis carried out based on the scores obtained make it possible to demonstrate that it is the purely clinical aspects and adaptation to the disease, and not the type of AF, that play a role in the direct impact on the HRQoL of the patients. The development of symptomatic episodes of AF, such as palpitations, dizziness/syncope, dyspnea, etc, would have, independently of the type of AF, a direct relationship to a reduction of the HRQoL of the patients, in accordance with similar studies in which both the development of symptoms in patients with AF19 and their control4,5 were evaluated.
Patients with a long history of AF, as is the case of permanent AF, which can remain stable over the course of time, with fewer symptomatic episodes, would have a better HRQoL in terms of the psychological dimension due to a reduction of the anxiety associated with this disease.18 Given that it has also been observed that there is a correlation between the number of visits to the emergency department and the deterioration in the HRQoL, according to the AF-QoL scores, it can be deduced that the higher the number of symptomatic episodes of the disease, as occurs in patients with paroxysmal AF, the greater their impact on the patient and the poorer his or her HRQoL, especially when considering the psychological aspect of this scale.
The HRQoL of the patients was also correlated with the functional class, according to the NYHA classification. In agreement with previous studies, the patients with a better functional class also have a better HRQoL.20
Finally, the treatment strategy had no direct relationship to the HRQoL in patients with AF, independently of the type of the disease. These findings would be in agreement with the results of the major clinical trials comparing the rate control and the rhythm control strategies in AF patients, in whom no statistically significant differences in HRQoL were observed regardless of the therapeutic strategy employed.21-23
CONCLUSIONS
The 3 types of AF were similar in terms of the HRQoL of the patients with this arrhythmia. However, patients with permanent AF are less affected (higher score) in the psychological dimension of the questionnaire, when compared with the scores of the patients with paroxysmal or persistent AF.
Patients with the most severe symptomatology, greatest number of visits to the emergency department, and worst functional class were those whose HRQoL was most affected, it being significantly reduced.
The AF-QoL questionnaire is a useful tool in the evaluation of the HRQoL of patients with AF, regardless of the type, since it enables the detection of differences in the HRQoL according to the clinical characteristics of the disease.
ACKNOWLEDGMENTS
The authors wish to express their appreciation for the work performed and the commitment made by all the centers, researchers, and patients that have participated in the study.

ABBREVIATIONS
AF: atrial fibrillation
AF-QoL: Atrial Fibrillation-Quality of Life
HRQoL: health-related quality of life
NYHA: New York Heart Association
SEE ARTICLE ON PAGES 1393-5
Funding: This study was made possible by the financial support of MEDA Pharma.
Correspondence: Dr. R. Peinado.
Sección de Arritmias. Servicio de Cardiología. Hospital Universitario La Paz.
P.º de la Castellana, 261. 28046 Madrid. Spain.
E-mail: rpeinado@secardiologia.es
Received August 4, 2009.
Accepted for publication June 14, 2010.