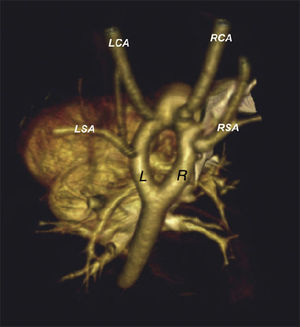
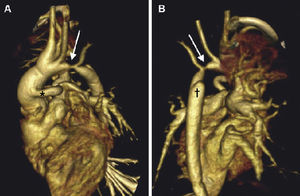
A 3-month-old male infant, with diagnosis of a complex, cyanotic, congenital heart disease (double-outlet right ventricle, pulmonary stenosis, and hypoplastic pulmonary arteries, among other defects) and a double aortic arch (Fig. 1, [L, left; LCA, left carotid artery; LSA, left subclavian artery; R, right; RCA, right carotid artery; RSA, right subclavian artery]), had required a shunt from ascending aorta to main pulmonary trunk (Fig. 2A, *), plus a section of the aortic arch distal to right subclavian artery (Fig. 2B, †).


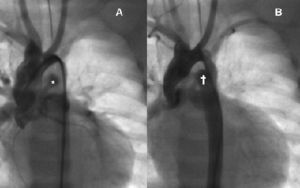
During admission, the infant experienced low systemic cardiac output, with arterial pressure gradient between upper and lower extremities, and an echo suspicion of aortic coarctation. A thorax computed tomography scan showed a stenotic area in the native, left aortic arch (Figs. 2A, 2B, arrow), bizarrely located between the left carotid artery and the left subclavian artery. Due to the atypical location of the coarctation, and the complexity and risk of the patient, after agreement with cardiac surgeons we accordingly performed a balloon catheter angioplasty to resolve the coarctation (Fig. 3A), which was effective and uneventful (Fig. 3B).

Angio computed tomography scan and 3D reconstructions provide fast, high-resolution images of congenital heart disease, with minimum radiation doses and use of intravenous contrasts. In infants with congenital heart disease, computed tomography scan is better than magnetic resonance imaging, especially in large-vessel anomalies. Findings may be later confirmed in the operation theater or the cath-lab. In our patient with double aortic arch intervention, computed tomography scan provided accurate images of an atypical coarctation, and allowed an individualized approach.
.