
Radiofrequency catheter ablation of the atrioventricular node (AVN) is the usual technique for rate control in patients with atrial fibrillation that is difficult to control with drug therapy, with positive results in up to 97% of patients. However, in isolated cases, it does not work.1
Alcohol ablation of the AVN artery was first described in 6 patients,2 after confirmation of transient atrioventricular block (AVB) with a selective infusion of cold saline, as described by Brugada et al.3 Other groups confirmed the safety and efficacy in short patient series, albeit with success rates limited to 72%.4 However, with the development of catheter ablation techniques, alcohol ablation fell into disuse.
We present the case of an 82-year-old woman, with hypertension, diabetes, and a previous inferior infarct treated with angioplasty of the circumflex artery, with a left ventricular ejection fraction of 47%. She had been admitted to hospital 1 year prior due to permanent nonvalvular atrial fibrillation poorly controlled on drug therapy. During admission, a synchronized pacemaker was implanted and AVN ablation was attempted but failed. She was admitted again with palpitations and dyspnea and was found to have atypical flutter with rapid ventricular response (figure 1A). A repeat attempt was made at AVN ablation via a right retrograde aortic approach, with Ensite Precision (Abbott) electroanatomical mapping, using an irrigated tip catheter with a contact sensor and a deflectable sheath. Since His bundle activation was not recorded, 50W applications were delivered guided exclusively by anatomy and electrograms, without success (figure 2A). It was decided to attempt alcohol ablation of the AVN artery. For this, selective infusions were performed: into the right coronary artery with no AVN artery identified, and into the left coronary artery, which showed a branch of the circumflex that appeared to course toward the anatomical area of the AVN (figure 2B,C). The left coronary artery was catheterized with a 3.5 EBU guide catheter and an angioplasty guidewire was advanced selectively to the AVN artery, advancing over it a 2.0 mm coaxial balloon catheter (figure 2D). Cold saline was selectively infused through this catheter, which resulted in transient AVB (figure 1B). Echo contrast was then injected to visualize the area perfused by this artery on transthoracic echocardiography, and we observed that the high part of the interventricular septum showed selective contrast uptake (figure 2E). With the balloon inflated to avoid backflow to the circumflex, 2 doses of 2mL each of 100% ethanol were infused, and immediately afterwards complete AVB and pacemaker rhythm was observed (figure 1C). Subsequently, selective contrast infusion via the coaxial catheter was performed, and distal amputation of the AVN artery (figure 2F) and no damage to the circumflex artery was observed. The procedure was considered finished after the absence of atrioventricular conduction for 30minutes (figure 1D). At follow-up, there were no complications. Peak high-sensitivity troponin T was observed (2.056 ng/L) during the 24hours following the procedure, and complete AVB persisted at 6 months.

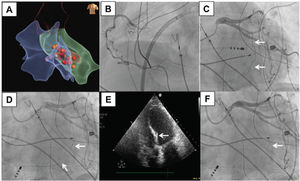
 artery and the area of the septum with contrast uptake. A: electroanatomical map (Ensite Precision, Abbott) showing the different radiofrequency applications from the right atrium, the coronary sinus, the right ventricle, and the left ventricle on an antero-posterior projection. B: right coronary artery on left anterior oblique (LAO) projection. C: left coronary artery (LAO projection; the arrow indicates the AVN artery). D: the arrow indicates the angioplasty guidewire and the coaxial balloon catheter in the AVN artery (LAO projection). E: echocardiography (apical view) during the selective infusion of echo contrast; the arrow indicates the area of the septum with uptake of echo contrast. F: left coronary artery after the selective injection of ethanol; the arrow indicates the amputated AVN artery (LAO projection).")
Coronary angiography and echocardiography from during the procedure. The arrows indicate, respectively, the atrioventricular nodal (AVN) artery and the area of the septum with contrast uptake. A: electroanatomical map (Ensite Precision, Abbott) showing the different radiofrequency applications from the right atrium, the coronary sinus, the right ventricle, and the left ventricle on an antero-posterior projection. B: right coronary artery on left anterior oblique (LAO) projection. C: left coronary artery (LAO projection; the arrow indicates the AVN artery). D: the arrow indicates the angioplasty guidewire and the coaxial balloon catheter in the AVN artery (LAO projection). E: echocardiography (apical view) during the selective infusion of echo contrast; the arrow indicates the area of the septum with uptake of echo contrast. F: left coronary artery after the selective injection of ethanol; the arrow indicates the amputated AVN artery (LAO projection).
AVN radiofrequency ablation with pacemaker implantation is a highly safe and effective method to achieve AVB, which allows the treatment of most patients with atrial fibrillation who have poor rate control (97% success in large series).1 In cases of failure, alcohol ablation of the AVN artery remains a valid alternative. In most people, the AVN artery originates in the right coronary artery, but in some (such as this patient) it can originate in the left coronary artery, and can occasionally be difficult to identify. Nonetheless, a detailed analysis on several projections usually allows identification of a branch running toward the center of the cardiac silhouette, corresponding to the AVN artery. Use of echocardiography for guidance and to help locate the area of the myocardium to be ablated has refined the technique compared with that described in early publications, ensuring greater safety and efficacy.
In conclusion, alcohol ablation of the AVN artery is a classic technique that should still be considered when radiofrequency ablation fails.