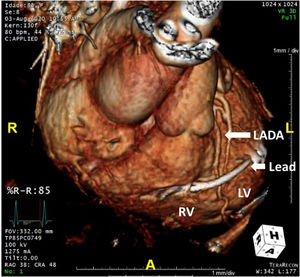
An 82-year-old woman was referred for lead extraction (LE) due to a pocket infection (informed consent obtained). LE was performed with the PISA approach (debridement was performed along the catheter, then the polypropylene dilation sheath was inserted and advanced externally to the catheter in rotational movements with a light traction of the catheter) without complications. During the new cardiac resynchronization pacing implantation and despite coronary sinus (CS) ostium identification, CS cannulation was impossible due to CS dissection related to the previous LE. In the catheterization attempt of the posterior interventricular vein, with a single smooth movement, the electrophysiology CS guiding catheter suddenly advanced into the left ventricle (LV). Contrast injection confirmed the sheath positioned in the LV. Transthoracic echocardiogram and radiological views suggested an iatrogenic interventricular communication in the anterior septum with no symptoms or acute hemodynamic impact. Considering the CS dissection, the stability of the patient and the access to the LV cavity in a patient under anticoagulation with warfarin due to atrial fibrillation, it was decided to implant an active lead in the lateral basal segment of the LV. Later, the patient developed cardiac tamponade requiring pericardiocentesis. A cardiac computed tomography angiography showed that the lead was implanted through an anterior right ventricular (RV) perforation, with a short epicardial path, crossing above the left anterior descending artery (LADA; figure 1, white arrows signal cardial structures), with the distal end lead localized in the endocardial lateral wall of the LV. Therefore, the lead withdrawal from the LV would have resulted in a catastrophic event, so it was not removed. The patient was discharged with a slight improvement in LV ejection fraction. To our knowledge, this case displays for the first time an endocardial LV pacing with this unexpected and highly unusual route.
FUNDING
No funding was received for this article.
AUTHORS’ CONTRIBUTIONSAll authors contributed equally in the procedure and clinical follow-up, as well as in the drafting of the present case report.
CONFLICTS OF INTERESTNone of the authors have any conflict of interest.
The authors are grateful for the support of the staff at the Cardiology Department of the Santa Marta Hospital, Lisboa, Portugal.