
Keywords
INTRODUCTION
The considerations regarding congenital anomalies of the coronary arteries has shifted in recent years. From simple coronary angiography findings of minor clinical importance, they are now known to be the cause of sudden death in youths and a possible cause of ischemia in the adult population.1,2
International forums have been calling for the creation of registries that include the group of coronary anomalies (CAs), to which are attributed most of the clinical events (sudden death and myocardial ischemia) occurring among the young and adult populations.3 Specifically, these anomalies include those originating in the contralateral sinus of Valsalva.
In order to describe this type of CA in a group of Spanish hospitals, the Registry of Coronary Artery Congenital Anomalies Originating in the Contralateral Sinus of Valsalva (RACES, Registro de Anomalías Congénitas de las Arterias Coronarias con Origen en el Seno de Valsalva Contralateral) was created among a group of 13 Spanish hospitals.
METHODS
The data recorded included congenital abnormalities originating in the contralateral sinus of Valsalva as well as single coronary arteries because these sometimes establish courses similar to those of CAs originating in the contralateral sinuses.
This was a prospective study in which each investigator, prior to the coronary angiography diagnosis of coronary anomaly, completed a questionnaire that included: patient age and sex, symptom for which the study was performed, description of the CA and its initial course, other diagnostic imaging methods used, presence of associated coronary disease (considered significant if >50% of total vessel lumen) and/or valvular disease, and treatment. Each hospital followed its usual diagnostic protocols. Informed consent was requested from each patient to be included. The study was conducted from 1 January to 31 December 2003.
RESULTS
Among 23 300 coronary angiographies, 98 CAs (incidence, 0.4%) were found to originate in the contralateral sinus (Table 1). Among the total studied, 70% were men (16 317) and 30%, women (6983). Among patients with CA, 70 were men (71%) and 28 women (29%). The mean age was 61.03±14.39 years (range, 16-87 years).

The most frequent indication for coronary angiography was angina (43.9%), followed by valve disease (20%), atypical pain (17.3%), acute myocardial infarction (14.3%), dyspnea (11.2%), syncope (1%), and dizziness (1%). No relationship was found between the type of CA and the presentation.
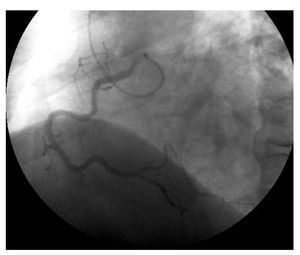
Forty-six circumflex arteries (Cx) (47%) originated in the right sinus of Valsalva (RSV) or right coronary artery (RCA), 25 RCA (25.5%) arose from the left sinus of Valsalva (LSV) (Figure 1), 10 left coronary arteries (LCA) (10.2%) originated in the LSV, 3 anterior descending arteries (3.1%) in the RSV, and 6 single coronaries (6.1%) and 8 CAs (8.2%) were included in the group of others (the anomaly was anatomically complex and could not be included in the above groups, but was characterized as originating in the contralateral sinus).

Figure 1. Coronary angiography showing a right coronary artery originating in the left sinus of Valsalva.
The initial course of the anomalous coronary was retroaortic in 36 (36.7%), anterior in 12 (12.2%), interarterial in 10 (10.2%), and "unknown" (or unidentified) in 40 patients (40.8%). The arterial course was diagnosed according to coronary angiography criteria (98%), with additional imaging used as a diagnostic method in only 2 cases.
Among the total of CA patients, 50 patients (51%) had associated coronary disease (in any coronary artery), but there was no relationship between the type of anomaly and the presence of coronary disease. Associated valve disease was found in 18%, and a statistically significant relationship was found between the presence of CA and aortic valve disease.
The CA was treated in 16.3% patients, most of them (15 patients) because of the presence of associated coronary disease. These cases were treated as any other atherosclerotic lesion, with no special considerations related to their anomalous course. Only one patient underwent surgery because of the anomaly.
DISCUSSION
The incidence in our registry was 0.4%, which is similar to previously published data.2,4-7 It is worth noting the difference in the number of CAs described between hospitals with a similar number of coronary angiographies (Table 1). We do not believe this is the result of any inherent differences between the populations in the autonomous communities of Spain. As has been observed by Angelini et al, the number of CAs described in each laboratory varies considerably due to the "meticulousness" of each group in the diagnosis.1,3
Once corrected for the total number of men and women undergoing catheterization, we found no gender-related differences in the incidence of CAs. As in most published studies, the Cx anomalies in our series (arising from the RSV or the origin of the RCA) were the most frequent2,8 (47%) (Figure 2).

Figure 2. Coronary angiography showing a circumflex artery that originates in the right sinus of Valsalva and takes a retroaortic course until reaching its point of normal distribution.
The initial course of the anomalous coronary, i.e., its anatomical relationship with the aorta and pulmonary artery, is an essential aspect when describing a CA, because certain courses (e.g., interarterial) are associated with a higher incidence of ischemia.9,10 One of the most interesting aspects of our registry was the almost exclusive use of coronary angiography to describe the initial courses. This may be the reason why the initial course was not identified in most patients (40.8%). Coronary angiography gives us a two-dimensional view of the coronary vasculature, a complex three-dimensional structure; hence other imaging methods are used to confirm or diagnose these courses (e.g., transthoracic or transesophageal echocardiography, magnetic resonance, or computed tomography).11-14 Nevertheless, in our registry, an additional technique was used in only 2 patients: transesophageal echocardiogram in one and magnetic resonance in the other. The course identified most often was retroaortic (36.7%), because of the predominance of anomalous circumflex arteries (these arteries tend to follow this course).2
The possible predisposition of the anomalous course of the CA to develop atherosclerotic disease was and is one of the more controversial points in CA studies. In fact, there appears to be an equal number defending each of the theories.2,8,15,16 In our registry, we observed associated coronary disease (in any coronary) in 51% of the cases, a finding consistent with the fact that most patients were referred for a study of ischemic heart disease with angina as the predominant symptom. However, we found no relationship between the presence of atherosclerotic disease and the different types of CAS (Table 2).

Aortic valve disease (primarily bicuspid) is known to be associated with CA, and this fact should be taken into account when considering potential surgery for this type of patient.17
Limitations of the Study
A specific joint protocol for CA diagnosis was not used in this registry. As a result, coronary angiograms were not analyzed by a core laboratory, but rather, different criteria were applied when establishing the diagnosis and describing the anomalous courses. Lastly, the use of additional imaging techniques was left to the discretion of each investigator.
The incidence of CA is similar to that reported in other series, showing a between-hospital variation possibly due to differences in "meticulousness" in the diagnosis of each group. There were no differences between men and women, and Cx anomalies were the most common. The initial course of the CAs was not identified in most cases, and an additional imaging technique was used in only 2 patients to diagnose this course. One patient was treated surgically only for the anomaly. We did not find a higher incidence of atherosclerosis in the anomalous courses, but did find an association between aortic valve disease and the presence of CA.
The RACES results are likely to indicate that we are not sufficiently aware of the potential prognostic importance of this condition because of its low incidence. We believe these data represent an extremely important starting point for the future establishment of diagnostic standards and protocols for CAs.
ACKNOWLEDGEMENTS
We thank Dr. Casariego for his support with the statistical analysis of the registry.
Correspondence:
Dr. R. Barriales-Villa.
Servicio de Cardiología. Complexo Hospitalario de Pontevedra. Hospital Montecelo.
Mourente, s/n. 36071 Pontevedra. España.
E-mail: rbarrialesv@inicia.es
Received December 29, 2004. Accepted for publication November 8, 2005.