To the Editor,
In recent years, transcatheter aortic valve implantation (TAVI) has been established as a safe and effective alternative for the treatment of severe symptomatic aortic stenosis in high surgical risk patients.1, 2 The selection of candidates is based on the use of risk scores (the EuroSCORE being that most widely utilized) that assess the associated comorbidities of each patient and quantify the surgical risk on an individual basis.3, 4.
In the population we attend to, certain patients are considered to be inoperable due to comorbidities secondary to the aortic anatomy, such as the existence of porcelain aorta, that are not included among the EuroSCORE variables. There are unconventional surgical alternatives (for example, the apicoaortic conduit), but they have yet to be employed in series of patients with an adequate follow-up period.2, 5, 6.
Porcelain aorta is a structural disease of the aortic wall defined as the extensive, circumferential calcification of the thoracic aorta, detected by means of computed tomography (CT) or fluoroscopy.3 The incidence of porcelain aorta in different series of patients with aortic stenosis treated with TAVI varies, and can be as high as 18%.2, 3 This circumstance and the poor vascular access are the two main reasons for considering transapical access in treatment with TAVI.3.
Little data has been published on the course of patients with porcelain aorta treated by means of TAVI with the Edwards Sapien device, but the limited available information appears to be favorable, although it has been shown to be associated with a higher rate of valve malposition, requiring reintervention to implant a new valve. Moreover, there is no evidence of an increase in cerebrovascular events in transapical implantation compared to the transfemoral approach.3, 4 With respect to the percutaneous implantation of the CoreValve® aortic valve prosthesis, there are no data on its use or on the postimplantation follow-up of patients treated for severe symptomatic aortic stenosis and porcelain aorta..
We report the cases of 2 patients with severe symptomatic aortic stenosis and porcelain ascending aorta, who were not suitable candidates for surgical valve replacement and were successfully treated by means of TAVI with a CoreValve® prosthesis via the transfemoral route..
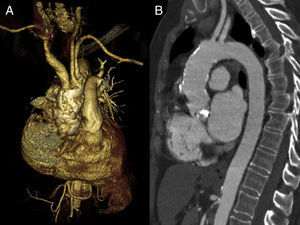
The first patient was a 72-year-old woman with no associated coronary artery disease and a logistic EuroSCORE of 2.9%. The peak and mean aortic gradients were 106mmHg and 68mmHg, respectively, and the diameters of the aortic annulus and ascending aorta, which was severely calcified, were 21mm and 30mm, respectively. Figure 1 illustrates the 3-dimensional reconstruction of the chest CT, showing that the calcification of the ascending aorta is severe, diffuse, and circumferential, characteristics that are all compatible with the diagnosis of porcelain aorta. Percutaneous implantation of a 26-mm CoreValve® prosthesis was successfully performed without complications; the presence of grade I/IV residual aortic regurgitation was verified by angiography. Echocardiographic evaluation 4 months after implantation revealed a peak gradient of 23mmHg, with mild aortic regurgitation..

Figure 1. Three-dimensional reconstruction (A) and chest computed tomography (B) showing severe, diffuse, circumferential calcification of porcelain aorta (first case).
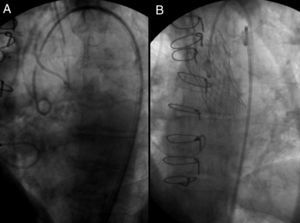
The second case was that of an 80-year-old woman with no associated coronary artery disease and a logistic EuroSCORE of 4.8%. The peak and mean aortic gradients were 126mmHg and 67mmHg, respectively, and the diameter of the aortic annulus was 23mm. She was initially accepted for surgical treatment, but after median sternotomy, evidence was observed of severe, generalized, circumferential calcification of ascending aorta that impeded clamping. Two months after this intervention, percutaneous implantation of a 29-mm CoreValve® aortic valve was successfully carried out without complications; grade I/IV residual aortic regurgitation remained. A follow-up echocardiogram performed 4 months later revealed a peak gradient of 17mmHg and mild aortic regurgitation. Figure 2 shows the fluoroscopic images in which severe calcification of ascending aortic wall and the correct position of the implanted prosthesis can be observed..

Figure 2. Fluoroscopic images showing severe calcification of ascending aorta (A) and the correct position (B) of the prosthesis (second case).
In the two cases reported here, it was possible to carry out the percutaneous implantation of the CoreValve® prosthesis following the standard protocol, as the difficulty of the technique was not incremented by the unfavorable anatomical conditions of the aorta.2, 6.
The clinical course has been favorable in both patients and after 6 months of follow-up they were asymptomatic and their functional status was excellent..
These 2 cases illustrate the positive results obtained with the percutaneous implantation of the CoreValve® aortic prosthesis in 2 patients with a low EuroSCORE and no associated comorbidities but with highly unfavorable aortic anatomies and, in 1 case, severe calcification which impeded surgical treatment..
Porcelain ascending aorta is a condition not considered among the variables in the conventional surgical risk stratification systems when applied to patients with severe symptomatic aortic stenosis, but it should be taken into account due to the fact that it impedes aortic clamping. We believe that percutaneous TAVI using the CoreValve® prosthesis may be a therapeutic alternative to be considered in these difficult to manage cases..
.
Corresponding author: cesarmoris@gmail.com