We present the case of a 91-year-old woman with severe symptomatic aortic stenosis. Computed tomography revealed a calcium nodule at the posterior aortic annulus.
Transcatheter aortic valve implantation (TAVI) was performed by predilating the native valve with a 23-mm balloon. An Edwards SAPIEN 3 prosthesis no. 26 was then implanted and, because there was persistent mild to moderate periprosthetic regurgitation, the valve was dilated with the same balloon, reducing the regurgitation to mild.
The initial clinical course was favorable but, some hours later, the patient developed hypotension with tissue hypoperfusion. Because of a suspected complication, we performed transthoracic echocardiography, revealing cardiac tamponade. Using pericardiocentesis, 450 cc of hemorrhagic fluid was extracted, with good results. Obnubilation started after 24hours, with no hemodynamic deterioration. Cranial computed tomography ruled out the presence of an acute condition explaining the symptoms. A few minutes later, she experienced cardiac arrest due to electromechanical dissociation and resuscitation was begun. Echocardiography revealed a pericardial hematoma that could not be percutaneously evacuated and the patient died.
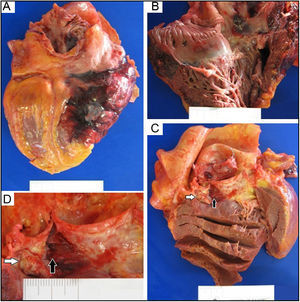
Autopsy revealed an intrapericardial hematoma compressing the right chambers, a transmural hematoma in the posterolateral region of the right atrium and ventricle (Figure, A and B), and a tear in the aortic subannular region between the noncoronary valve and the right coronary artery (Figure, C and D, black arrows), near a calcium nodule (Figure, C and D, white arrows).

The insidious clinical presentation of this rare complication was the result of an aortic subannular rupture generating an intramural hematoma and subacute cardiac tamponade. This condition might have been related to valve implantation with an expandable balloon or to predilatation and postdilatation of an annulus with nodular and asymmetric calcium.