
Keywords
INTRODUCTION
Fungal endocarditis forms an estimated 2%-6% of all endocarditis1 and less than 1% of fungal endocarditis occurs in pacemaker carriers.2 Diagnosis is difficult and when the infecting fungus is Aspergillus fumigatus mortality can be >90%.3 We present the case of a female pacemaker carrier who developed fatal A fumigatus endocarditis.
CLINICAL CASE
Seventy-four-year-old woman with a bicameral pacemaker implanted 5 years earlier. Five months before admission she began to present intermittent fever and shivering. Physical exploration was normal whereas blood analysis showed modest white cell count and high ESR (105 mm); serology, antibodies and tumor markers were normal. Transthoracic echocardiogram did not show vegetations. Chest x-ray showed calcification compatible with granuloma in right upper lung (RUL) lobe; 2 months later a new mass appeared next to the calcification. Computerized thoracic tomography (CT) showed a 15-mm calcified granuloma together with small infiltrates attached to the RUL and left lung, and right pleural swelling. Sputum culture and a series of 3 Ziehl-Neelsen smears were negative despite which tuberculostatic treatment was started. One month later the patient again presented fever leading to her being hospitalized for further study.
Mobile images compatible with vegetations adhering to the pacemaker lead were observed with transesophageal echocardiogram. On the second day following admission, Staphylococcus hominis was isolated in 2 blood cultures and antibiotic treatment was initiated with vancomycin, rifampicin, and gentamycin. One week later, due to the persisting fever, she underwent surgery and the pacemaker, its leads, and numerous vegetations in the right cavities removed. A new epicardial pacemaker was implanted. Anatomopathological study showed abundant fungal hyphae, compatible with Aspergillus, that also grew in the blood cultures. Treatment started with intravenous liposomal amphotericin B while continuing antibiotic treatment for Staphylococcus. Complications arose due to Escherichia coli pneumonia, septic shock, right-sided heart failure, and kidney failure. Ten days later the patient died.
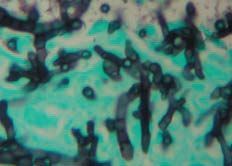
The autopsy revealed a large embolus encased in the right ventricle occluding the pulmonary trunk and both branches of the pulmonary artery (Figure 1). Histological study showed the presence of a large amount of Aspergillus spores and hyphae in this thrombus (Figure 2), granulomatous arteritis with giant cell reaction in the presence of fungus, aspergilloma in the left lung, and multiple pulmonary microemboli in different stages of development and acute bilateral broncopneumonia foci.

Figure 1. Heart with a large thrombus encased in the right ventricle that extends to and occupies the trunk of the pulmonary artery.

Figure 2. Histological section of the thrombus showing abundant branched and septate hyphae forming part of the thrombotic material (hematoxylin-eosin).
DISCUSSION
The present case is unique due to the following factors: the difficulty involved in its diagnosis despite following a strict diagnostic protocol; Aspergillus infection is the least frequent pacemaker endocarditis3; and, as in our case, the diagnosis was made mainly with the material extracted from the infected lead4 or during necropsy.5
Vegetations easily become emboligenic, as suggested in our patient by the thoracic TC lung images and confirmed by necropsy. Transthoracic echocardiography did not lead to the diagnosis during the first examination, whereas transesophageal echocardiography was useful in this regard some months later. The fatal outcome is consonant with the high mortality referred to, despite having used the recommended surgical treatment plus medical treatment with amphotericin B.6
Our patient had all the characteristics presented by this fungal infection, such as diagnostic delay despite following a rigorous diagnostic protocol for febrile syndrome, the long duration of the symptoms before hospitalization, the initial negative results in blood cultures, the presence of extracardiac manifestations in the form of septic embolizations, and the death of the patient as the final outcome following a desperate attempt at treatment.
Correspondence: Prof. J.R. Berrazueta.
Servicio de Cardiología. Hospital Universitario Marqués de Valdecilla.
Avda. Marqués de Valdecilla, s/n. 39008 Santander. Cantabria. España.
E-mail: jose.berrazueta@unican.com
Received March 24, 2004.
Accepted for publication October 5, 2004.