


Calcified nodules (CN) have been associated with higher complexity and worse outcomes after percutaneous coronary intervention (PCI) in both stable and unstable coronary disease. The aim of this systematic review was to summarize the current evidence on CN.
MethodsSystematic review of published studies on the prevalence, clinical associations, and impact of CN on outcomes after PCI up to November 2024.
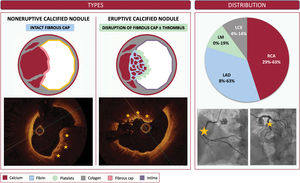
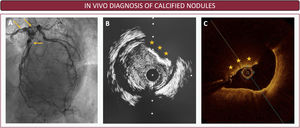
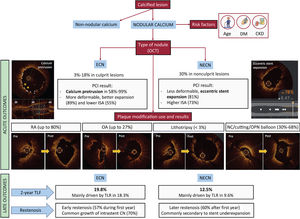
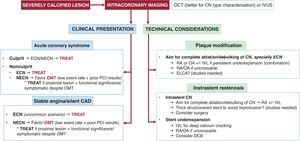
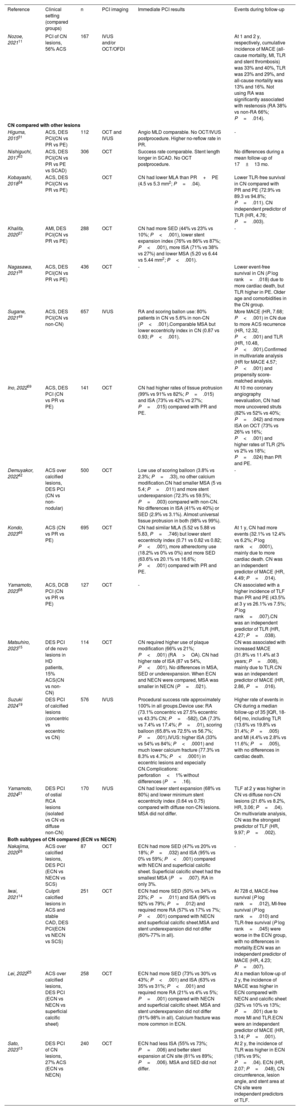
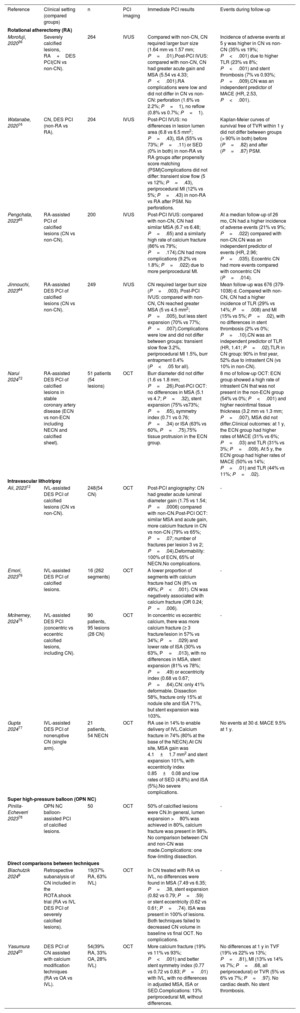
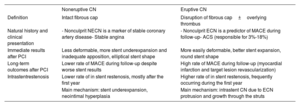
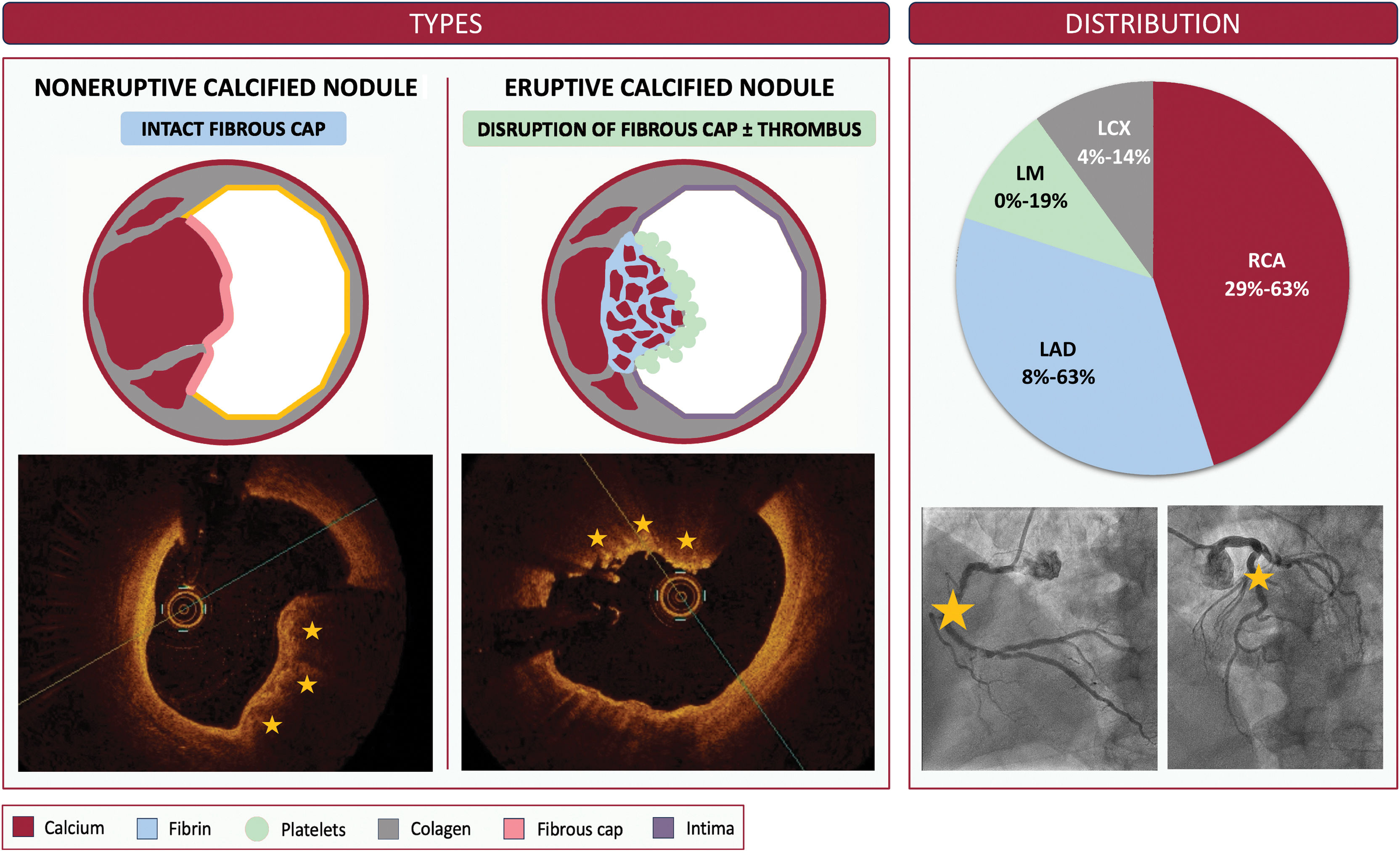
ResultsWe identified 474 publications, of which 87 were included (all observational). CN were divided into 2 types: noneruptive CN (NECN), with an intact fibrous cap; and eruptive CN (ECN), with disruption of the fibrous cap with or without thrombus. The most common location was the right coronary artery (28%-71%). Angiography-based diagnostic sensitivity was low (18%-38%). Optical coherence tomography was preferred for type differentiation. The main clinical factors associated with CN were older age, diabetes mellitus, and chronic kidney disease. CN were considered the culprit lesion in 3% to 18% of acute coronary syndromes but were also present in up to 30% of nonculprit arteries. ECN were associated with more events at follow-up than NECN (20% vs 3.3% at 1 year). Post-PCI, CN were associated with lower minimum lumen area (MLA), higher rates of stent-edge dissection (44%-73%), malapposition (71%-96%), and underexpansion (60%-77%). ECN were associated with better acute results but worse long-term outcomes compared with NECN.
ConclusionsCN are often present in acute coronary syndrome culprit and stable coronary lesions. Intracoronary imaging is essential for the diagnosis and differentiation of CN. CN are associated with worse outcomes after PCI, acutely and during follow-up.
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm