To the Editor,
We have read with great interest the article by Cortell et al1 in which the authors analyze the data of 64 patients with a presumed non-ST elevation acute myocardial infarction (NSTEAMI) with coronary arteries with no significant lesions. These authors find certain predictors of normal coronary arteries for patients with NSTEAMI which are highly coincident with the CPU-65 index (comorbid diabetes, typical pain, use of aspirin and age 65 years or more) that we described 5 years ago after analyzing the data from the chest pain unit of our center.2 A CPU-65 index equal to zero makes it possible to rule out the presence of coronary artery disease, with a negative predictive value of 99.9%3 and, even in the case of patients with a positive ischemia test, 80% have normal coronary arteries.4 However, we are surprised that the authors do not include the characteristics of the pain as predictors of a lesion-free coronary angiography. In our series, typical chest pain doubled the probability of significant coronary artery disease and, as a result, sex was no longer an independent predictor. We would like to know if the opposite occurred in the series of Cortell et al or whether the pain characteristics simply were not recorded.
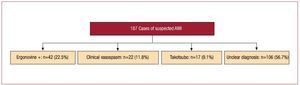
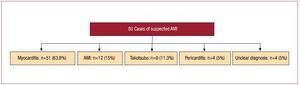
On the other hand, we are not sure that all the patients in the series of Cortell et al. Had had an acute myocardial infarction (AMI) and we are also surprised by the fact that the authors provide no data on the incidence of coronary vasospasm. Recently, we published the data of the VIRIATO (Vasospasm Incidence Registered After Investigation with Angiography and Tested Objectively with Ergonovine) registry, which included 346 consecutive patients from our center with suspected acute coronary syndrome and coronary arteries with no significant lesions.5 If we focus on the 187 patients with elevated troponin T levels, the majority without ST elevation, at least 9% of patients did not have an AMI, but takotsubo stress cardiomyopathy6 (Figure 1). The new studies with cardiac magnetic resonance seem to demonstrate that most of the patients with suspected AMI but no significant coronary artery lesions, in reality, have myocarditis.7-9 The series of Laraudogoitia Zaldumbide et al,7 with a clear predominance of patients without ST elevation, is particularly demonstrative in this respect (Figure 2).

Figure 1. Final diagnosis in the 187 patients of the VIRIATO (Vasospasm Incidence Registered after Investigation with Angiography and Tested Objectively with Ergonovine) registry with elevated troponin T concentrations.5,6 Unclear diagnosis: diagnosis not clarified at the time of hospital discharge; ergonovine +: positive spasm provocation test with methylergonovine; AMI indicates acute myocardial infarction; takotsubo, takotsubo stress cardiomyopathy; clinical vasospasm, highly typical event that was ultimately treated with calcium channel blockers.

Figure 2. Final diagnosis in the 80 patients of the series of Laraudogoitia Zaldumbide et al.7 AMI indicates acute myocardial infarction; takotsubo, takotsubo stress cardiomyopathy; unclear diagnosis, diagnosis not clarified at the time of hospital discharge
We consider the data of Cortell et al to be very interesting as they help to identify patients with suspected NSTEAMI whose coronary arteries show no significant lesion, but we think that the absence of these lesions should lead us to reconsider the initial diagnosis in many patients.