We read with interest the letter by Alconero-Camarero et al about our article, “Analysis of Telephone Calls to a Heart Failure Unit: Reasons for the Call and Resource Use,”1 and we would like to make certain clarifications.
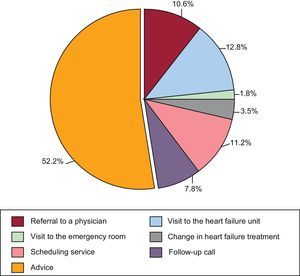
Our study merely refers to an assessment of the reasons for spontaneous telephone calls made by patients. The attention provided by telephone was not subject to a prior protocol. Likewise, the nurses’ responses were not standardized (Figure) and, as was stated, depended on the type of consultation. Obviously, this activity is complementary to other more important activities undertaken by the unit (education, supervision, treatment optimization, care for cases of decompensation, etc.). In no way should this task be compared with care programs or telephone-based follow-up of patients referred to by Alconero-Camarero et al.

We do not believe that our results indicate the telephone calls can be attributed to the lack of prior educational intervention in the patient’ treatment plan. They simply highlight that, among all the calls made, the main causes are related to treatment. Often, the caller was seeking a positive reinforcement, that is, confirmation of aspects dealt with in the educational intervention. In fact, although the concept of self-care includes a dimension of self-management, it is also important to know when to contact health care professionals. We also do not share their opinion that greater confidence in the staff of the unit and their accessibility, a crucial aspect of heart failure units, are in conflict with promoting self-care, as the authors suggest. On the contrary, it can be considered a mechanism of self-care and encourages greater vigilance on the part of the patient.
We do agree, however, that the number of bureaucratic questions answered by nurses is worthy of attention, and this was behind our comment in the article.
Finally, we are (and have provided sufficient evidence of being) staunch supporters of a multidisciplinary approach and integration of other levels of care, such as primary health care, without this being mutually exclusive with facilitating as much as possible patient access to heart failure units.