We present the case of an 80-year-old man who underwent successful mitral valve replacement with a biological prosthesis. Predischarge transthoracic echocardiography showed a mitral bioprosthesis with normal gradients, without residual regurgitation.
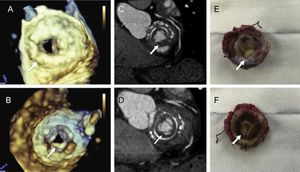
Less than a year later, the patient reported exertional dyspnea. Transthoracic echocardiography was performed and showed severe prosthesis dysfunction with moderate regurgitation and a high mitral inflow mean gradient of 20 mmHg. Transesophageal echocardiography showed extensive tissue ingrowth encroaching into the supravalvular mitral inflow orifice (arrow points to atrial side [Figure A] and ventricular side [Figure B]), causing restricted mobility of the leaflets and significant stenosis of the mitral prosthesis orifice. Cardiac computed tomography was performed to discriminate the tissue. It depicted extensive, homogeneous periannular tissue ingrowth on the left atrial and ventricular side compatible with pannus (arrow points to atrial side [Figure C] and ventricular side [Figure D]).

Surgical resection was performed. The intraopearative description of the resected bioprothesis was a tissue ingrowth compatible with pannus in both the atrial (Figure E) and ventricular side (Figure F) causing restricted leaflet mobility. Histological study confirmed pannus prosthetic valve obstruction.
In conclusion, the detection, evaluation and treatment of prosthetic valve obstruction are challenging. Rapid pannus ingrowth, although infrequent in the early postoperative period, should be considered when a patient presents with a progressive increase of the mitral inflow gradient after valve replacement. Nowadays it is critical to understand the strengths and weaknesses of each imaging modality to select the most appropriate and cost-effective test for each patient. Cardiac computed tomography may serve as an adjunct to echocardiography and it may provide additional information to establish the diagnosis and guide treatment in this setting.