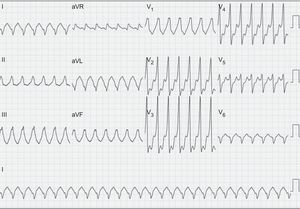
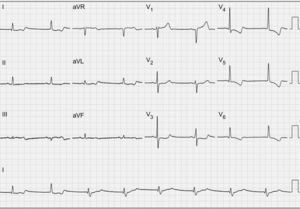
A 62-year-old man presented to the emergency room with palpitations and dyspnea. The patient had a history of kidney disease and bicuspid aortic valve disease, with class III/IV heart failure and left ventricular dilatation and dysfunction (ejection fraction, 40%) but no history of palpitations, dizziness, or syncope. Physical examination on admission revealed blood pressure of 130/80 mmHg and no overt signs of heart failure. The admission ECG showed regular, wide-QRS tachycardia (Figure 1). Sinus rhythm was restored with electrical cardioversion (Figure 2).What is the most mechanism in this patient?
- 1.
Monomorphic ventricular tachycardia due to myocardial reentry.
- 2.
Monomorphic ventricular tachycardia due to bundle branch reentry.
- 3.
Nodal reentrant tachycardia with right bundle branch block.
- 4.
Preexcited tachycardia.


Suggest a solution to this ECG Contest at http://www.revespcardiol.org/es/electroreto/70/4. The answer will be published in the next issue (May 2017). #RetoECG.