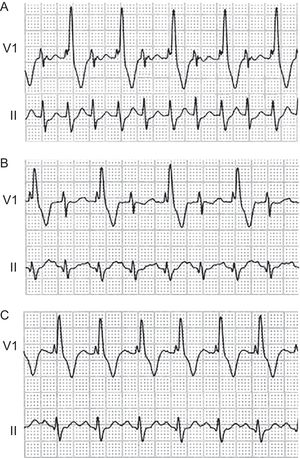
A 55-year-old woman was admitted to the emergency room for palpitations. Analysis of the ECG (Figure, panel A) showed a regular tachycardia (190 bpm) with alternation of narrow and wide QRS complexes (right bundle branch block [RBBB] morphology). The R-R intervals were stable. Narrow QRS beats showed a pseudo-r’ wave in V1, suggesting slow-fast atrioventricular nodal re-entry tachycardia. The patient was hemodynamically stable (blood pressure 130/80mmHg). Vagal maneuvers were ineffective. Adenosine was administered in intravenous bolus (6mg), obtaining sinus rhythm restoration (Figure, panel B, in lead II a clear positive P wave was observed). The ECG after cardioversion showed sinus tachycardia 140 bpm. Alternation of narrow and wide QRS complex persisted. Curiously, after some minutes, this singular behavior ceased, along with heart rate slowing (120 bpm, Figure, panel C). The final ECG showed sinus tachycardia with constant RBBB.

How do you explain alternation of narrow and wide QRS complexes in panel A and B?
- 1)
Bigeminy ventricular extrasystoles with constant fusion beats.
- 2)
2:1 RBBB.
- 3)
Phase 4 RBBB.
- 4)
RBBB, supernormal conduction and linking phenomenon.
Suggest a diagnosis to this ECG Contest at http://www.revespcardiol.org/en/electroreto/71/02. The answer will be published in the next issue (February 2018). #EKGchallenge.