To the Editor:
Surgery for acute type B aortic dissection (ABAD) is complex and has a high risk of morbidity and mortality. Endovascular stent-grafting has recently begun to be used in acute aortic syndrome with promising short-term and mid-term results.1-4 In certain cases, severe atherosclerotic degeneration of the iliofemoral and iliac axis may constitute a contraindication for stent-graft implantation.1 We present a case of endovascular stent-grafting for uncomplicated ABAD performed through the ascending aorta and without extracorporeal circulation in a patient with peripheral vascular disease and a high probability of aortic rupture during follow-up.
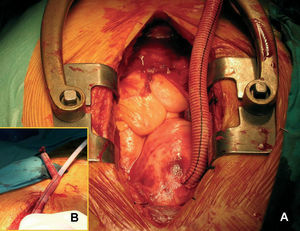
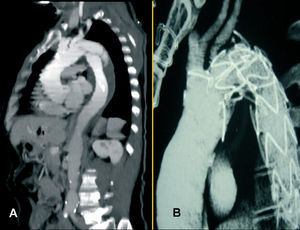
A 58-year-old man, smoker, with hypertension, and hypercholesterolemia came to the emergency room with a two hour history of central chest pain with sweating and nausea. The chest x-ray showed mediastinal widening, aortic elongation, and absence of pleural effusion. The myocardial necrosis enzymes were normal. CT angiography revealed an aortic dissection from 1 cm below the origin of the left subclavian artery to the iliac bifurcation, with a maximum aortic diameter of 42 mm and severe calcified atherosclerosis of the abdominal aorta and the iliofemoral axis (Figure 2). Catheterization showed significant lesions in the distal circumflex, right iliac, and left common femoral arteries. The intravascular ultrasound with a 9 Fr, 9 MHz Ultra ICE catheter, and Galaxy imaging system (Boston Scientific Corporation, Wayne, New Jersey, United States) confirmed that the primary entry tear was distal to the left subclavian artery origin and the partially patent false lumen. Eleven days after the diagnosis, the patient underwent endovascular stent-grafting by midline sternotomy, but with no extracorporeal circulation. The anterior wall of the ascending aorta was clamped laterally and a 10-mm Hemashield PlatinumTM (Boston Scientific Corporation, Wayne, New Jersey, United States) graft was sutured end-to-side to the aorta (Figure 1A). This was used to implant a Talent stent-graft of diameter 38 mm and length 11.4 cm (Medtronic/AVE, Santa Rosa, California, United States) (Figure 1B). Follow-up aortography revealed residual flow through the entry tear that partially filled the false lumen and, therefore, a thoracic extension of diameter 38 mm and length 4.6 cm was implanted proximally. The postoperative period was uneventful. CT angiography before discharge showed complete occlusion of the entry tear with no filling of the false lumen, whereas the left subclavian artery showed only partial filling (Figure 2). At 7 days from the procedure, the patient was discharged with absence of left radial pulse, but no evidence of ischemia, and 3 months later he remained asymptomatic.

Figure 1. Intraoperative image. A: Hemashield PlatinumTM end-to-side ascending aorta graft. B: advancing the endovascular stent-graft.

Figure 2. CT angiography reconstruction: preoperative (A) and postoperative (B).
Endovascular stent-graft placement has emerged in recent years as an alternative to surgery in complicated ABAD, in which the entry tear is closed in 90% to 100% of cases.1,2 The case we describe represents an example of the use of endovascular stent-grafting in ABAD with no evidence of rupture, a strategy we believe is justified in selected cases. The mid-term prognosis of uncomplicated ABAD treated conservatively is poor, with mortality occurring in 27%, false lumen aneurysm in 14% to 20%, need for deferred surgery in 13%, and a 5-year incidence of serious complications of 33%.5 An aortic diameter larger than 40 mm and the presence of a patent false lumen in the acute stage have been identified by multivariate analysis as predictive factors of chronic aortic dilatation and major events during follow-up.4-7 In our case, we considered that the patient's poor progress, combined with the coexistence of risk factors, persistence of a partially patent false lumen, and borderline aortic diameter, justified endovascular stent-grafting to prevent a fatal event. To date, the scientific evidence for this strategy is not consistent. Currently ongoing studies must be completed, including larger series with longer follow-up, before we can identify patients who may benefit from an early interventional strategy.
Calcified atherosclerotic lesions in the iliofemoral axis are a relative contraindication for endovascular stent-grafting because of the difficulty and risk involved in advancement of the stent-graft.1 The abdominal aorta, aortic arch, axillary artery, and carotid artery are possible alternative routes. Our patient presented severe calcification in the abdominal aorta and, therefore, we ruled out this approach. The technique for implantation of an endovascular stent-graft through the ascending aorta without extracorporeal circulation was described by Abad et al,8 who used it successfully in a patient with descending aortic aneurysm. Working through an end-to-side aortic graft allows the material to be inserted without damaging the wall and facilitates hemostasis once the procedure is concluded. We believe this method is preferable to the direct aorta catheterization described by deRose et al,9 and our case demonstrates that it is applicable in ABAD. The technique has the added advantage that the stent-graft is inserted in a segment of healthy aorta and advances in an anterograde manner, thus lowering the risk of retrograde dissection and, at least initially, providing certainty of placement through the true lumen.