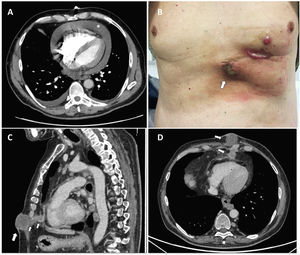
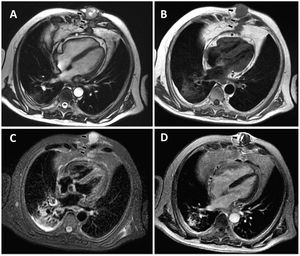
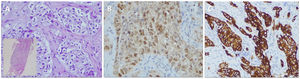

A 59-year-old man presented to the emergency department due to syncope and dyspnea. Thoracic computed tomography (CT) showed a tumor around the right main bronchus and a severe pericardial effusion (figure 1A; asterisk). Urgent ultrasound-guided subxiphoid pericardiocentesis was performed. The cytology of the pericardial fluid was positive for malignant cells and the pericardial catheter was removed after 24hours. Endobronchial biopsy confirmed the diagnosis of pulmonary adenocarcinoma. Several months later, the patient noted a growing subcutaneous nodule (figure 1B; arrow). A new CT showed a subcutaneous mass in the anterior thoracic wall and 2 nodules in the anterior pericardial fat, following the trajectory of the pericardial catheter (figure 1C,D; arrows). Cardiac magnetic resonance (CMR) confirmed the presence of nodules in contact with the pericardium, as well as a subcutaneous mass (figure 2A; asterisk and arrows). CMR tissue characterization showed that the lesions were isointense in the T1-weighted sequence (figure 2B; arrows) and hyperintense in the T2-weighted sequence (figure 2C; arrows). Finally, postcontrast study demonstrated peripheral late gadolinium enhancement (figure 2D; arrow). Although there was no specific pattern of metastasis, these findings were highly suggestive of secondary tumor spread. Biopsy of the subcutaneous nodule revealed malignant cells (figure 3A) and immunohistochemical analysis revealed expression of TTF-1 (figure 3B) and cytokeratin 7 (figure 3C) compatible with lung adenocarcinoma metastasis.



Tumor seeding after pericardiocentesis is a rare complication, and has been most frequently described after gastrointestinal interventions. This is an exceptional and well-documented case of iatrogenic pulmonary adenocarcinoma metastasis after pericardiocentesis.
All information/images have been anonymized. The patient gave his verbal consent before dying and the local ethics committee approved the case as a publication.
FUNDINGNone declared.
AUTHORS’ CONTRIBUTIONSThe first and last author participated in collecting the information and editing the manuscript and figures. The second author confirmed the histological diagnosis and edited the biopsy images.
CONFLICTS OF INTERESTNone.