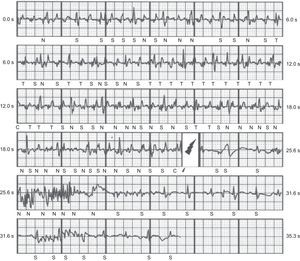
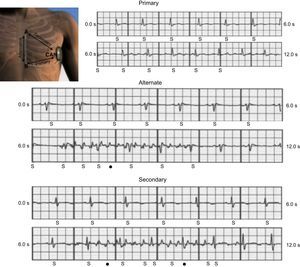
We would like to call attention to the case of a 32-year-old woman that was admitted to our hospital after a subcutaneous implantable cardioverter defibrillator (ICD) shock. One month earlier she underwent implantation of an entirely subcutaneous ICD (Boston Scientific Inc., Natick, Massachusetts, United States) in the setting of secondary prevention and familial long QT syndrome. No other episodes of sudden death were reported in her family and after first degree familial screening it was found that her mother also had a long QT interval. At implantation, a satisfactory position of the subcutaneous lead was achieved and therapies were programmed over 200 beats per minute for the conditional shock and 220 beats per minute for the shock zone. It was found during device interrogation that an inappropriate shock was delivered secondary to external noise detection that was interpreted as tachycardia (ventricular tachycardia/ventricular fibrillation) (Figure 1). The patient reported that prior to the shock she started clapping and after 15 to 30seconds felt the electric shock. For that reason we tried to reproduce the external noise while clapping and discovered that 2 of the 3 possible sensing vectors (secondary and alternate) reproduced it systematically. Luckily it was almost imperceptible with the primary sensing vector (Figure 2).


The overall incidence of inappropriate shock deliveries in subcutaneous ICDs varies in different series from 4%1 to 25%.2 It has been reported that such shocks can decrease quality of life or increase mortality in these patients.3,4 Whether such findings also occur with subcutaneous ICDs still has to be proven. In the Weiss et al study,5 inappropriate shock delivery was comparable to such incidence among intravascular ICDs, but with fewer supraventricular tachycardias and more T-wave oversensing. The use of the conditional zone (rate plus discriminators) also led to fewer inappropriate shocks.5 In general, it has been reported that T-wave oversensing is the most common cause for inappropriate shocks from subcutaneous ICDs5. Aside from T-wave oversensing and supraventricular tachycardias, broad QRS complexes and noncardiac oversensing have been reported as exceptional reasons for inadequate shocks.6 Interestingly, in the Weiss et al study 3 patients received an inappropriate shock as a result of external noise while working with electrical equipment.
We describe another possible cause of inappropriate shocks secondary to myopotentials oversensing that has not been previously reported. It was very interesting that the external noise was only present when the sensing vectors were using the tip of the cable (alternate and secondary sensing vectors). We postulate that pectoral muscular contractions during clapping produced myopotentials interference specifically in this part of the cable and that it caused the external noise that was interpreted as tachycardia/ventricular fibrillation. It has been emphasized that T-wave oversensing must be avoided during device implantation, using any of the 3 possible sensing vectors. After this finding, we are going to check for myopotentials after repetitive and rhythmic contractions in our patients, even though no prior situation has been reported in the literature and this is probably an uncommon cause of inappropriate shock. Since this is a relatively new technology and subcutaneous ICDs programming and follow-up is somewhat different compared to conventional ICDs, we recommend that other clinicians look for myopotentials and choose the vector with fewer artifacts and better T-wave sensing.