Lactococcus garvieae has previously been reported as a major pathogen in the aquaculture environment with low virulence for humans. Nevertheless, various episodes of human infections have been described in the literature. We report the first 2 cases of Lactococcus garvieae infective endocarditis (IE) in the Spanish population.
The first patient is a 70-year-old woman without cardiovascular risk factors who was admitted because of progressive heart failure without registered fever or infectious symptoms. Physical examination revealed a previously unknown holosystolic murmur in the apex irradiating to the axillae. Anemia, leukocytosis, and elevated C-reactive protein levels were detected at admission.
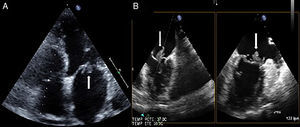
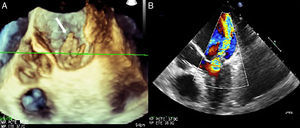
Intravenous diuretic therapy was initiated with good response. Blood cultures were performed (×4) and empirical antibiotic therapy was initiated with amoxicillin-clavulanic acid plus gentamicin. Transthoracic echocardiography showed 2 vegetations attached to the anterior and posterior mitral leaflets with severe mitral regurgitation. Blood cultures were all positive for Lactococcus garvieae sensitive to cefotaxime, ciprofloxacin, erythromycin, daptomycin, and vancomycin. Antibiotic therapy was switched to vancomycin. There was no history of raw fish consumption prior to admission or gastrointestinal disorders. New transthoracic (Figure 1A) and transesophageal (Figures 1B and 2) echocardiography were performed, showing several vegetations attached to both the posterior and anterior mitral leaflets with severe mitral regurgitation and severe pulmonary hypertension. Because heart failure treatment was ineffective, the patient underwent urgent cardiac surgery and a biological prosthesis was implanted (Mosaic N°27). After 6 weeks on intravenous antibiotic therapy, she was discharged and 1 year later remains asymptomatic and without relapsing IE episodes.
.")
. B: Transesophageal echocardiography showing severe mitral regurgitation.")
The second patient is a 77-year-old woman with a history of hypertension, chronic lymphatic leukemia, and colorectal cancer surgery complicated with Lactococcus garvieae bacteremia who was admitted 2 months after colorectal surgery due to persistent back pain and fever. X-ray, bone gammography, and magnetic resonance imaging showed inflammatory disease involving the L4-L5 vertebrae and paravertebral soft tissues. Blood cultures were positive for Lactococcus garvieae. Transesophageal echocardiography showed severe aortic stenosis without signs of IE. There was no history of raw fish consumption prior to admission and the patient was managed with outpatient parenteral antimicrobial therapy.
Three months later she was admitted due to purpuric lesions, physical discomfort, and fever within the last 48hours and acute renal failure (creatinine, 3.24mg/dL). Blood cultures (×3) were positive for Lactococcus garvieae sensitive to penicillin, amoxicillin-clavulanic acid, ciprofloxacin, and vancomycin. A transesophageal echocardiography showed vegetations attached to the aortic and mitral valves with severe aortic stenosis, severe mitral regurgitation, and severe pulmonary hypertension. Intravenous diuretic and antibiotic therapy with ampicillin plus gentamycin was initiated and skin biopsy of the purpuric lesions showed leukocytoclastic vasculitis. Surgery was ruled out due to the patient's high surgical risk and finally the patient died due to heart failure resistant to medical treatment.
The Lactococcus genus belonged to the Streptococcus genus due to its microbiological characteristics until 1985, when, with the help of genetic analysis of DNA and 16S rRNA sequencing data, the former Lactic acid streptococci became known as Lactococcus.1 There are 8 recognized Lactococcus species, of which Lactococcus lactis and Lactococcus garvieae are the most frequently found in human infections.2
Lactococcus garvieae is a Gram-positive, catalase-positive, facultative anaerobic cocci grouped in short chains. Although previously described as a major pathogen in the Asian aquaculture environment, it has been recognized as an emerging zoonotic pathogen, with several cases of infection in humans having been reported in the last few decades.3Lactococci can be misidentified as Enterococci due to problems with phenotypic methods and therefore the incidence of infections in humans may be higher than previously reported.3 The identification of this microorganism has been improved by 16S rRNA gene sequencing. Regarding its antimicrobial sensitivity, it has been shown to be resistant to clindamycin and sensitive to penicillins and aminoglycosides.4
Lactococcus garvieae has been related to different opportunistic infections in humans: bacteremia, IE, osteomyelitis, liver abscess, and peritonitis. The exact mechanism leading to infections in humans is not well-established but has been related to gastrointestinal disorders, such as colonic polyposis and diverticulosis and raw fish consumption.5 The most common infectious disease related to this microorganism is IE. To date, only 13 cases have been published on IE due to this microorganism. Of these, 46% occurred in Asia, 62% in males, and 69% were native IE episodes. Gastrointestinal disorders were present in 5 cases (38%) (3 colonic polyposis, 1 colonic diverticulosis, 1 gastric ulcer) and 46% had a history of prior raw fish/bone fish consumption. The clinical course was good with intravenous penicillins and/or aminoglycosides for 6 weeks. Six patients required cardiac surgery (46%) (4 urgent and 2 elective after hospital discharge due to the residual effects of the IE). Unlike previous mortality rates related to IE among the Spanish population (30%),6 in-hospital mortality due to this microorganism was low (8%), with 1 death being due to massive intracranial bleeding and another death occurring 3 weeks after hospital discharge due to unidentified causes.