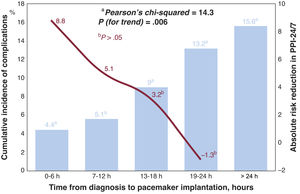

Most of the complications associated with acute and symptomatic bradyarrhythmia (ASB) occur in the time from diagnosis to permanent pacemaker implantation (PPI). We aimed to evaluate the outcomes of an urgent 24/7 PPI service (PPI-24/7) for patients with ASB.
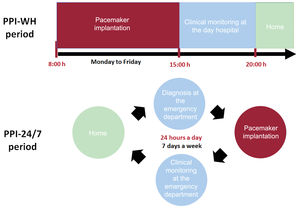
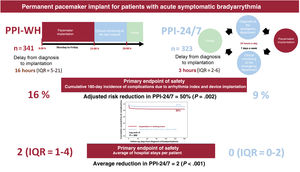
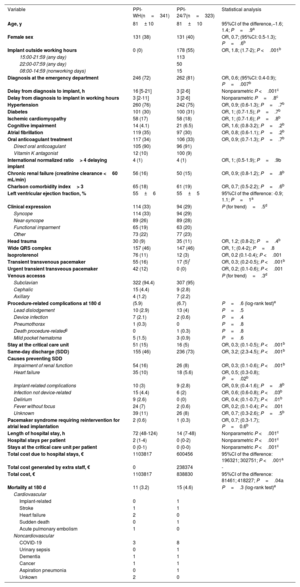
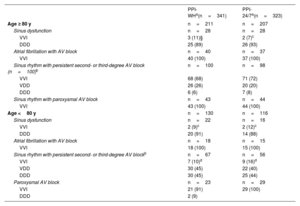
MethodsA total of 664 patients undergoing first-time PPI for ASB were prospectively assessed during 2 periods of identical length (18 months): 341 patients who underwent the procedure during working hours only (PPI-WH), and 323 patients who underwent the procedure after the implementation of the PPI-24/7 service. The primary safety endpoint was established as the cumulative 180-day incidence of complications related to the index arrhythmia and device implant. The primary efficacy endpoint was determined as the average number of hospital stays per patient.
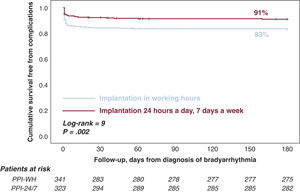
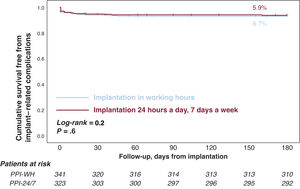
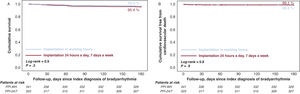
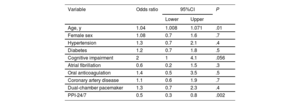
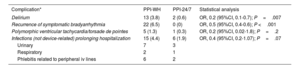
ResultsThe PPI-24/7 period was associated with a significant shortening of the time from diagnosis to implantation (median [interquartile range]): 3hours [2-6] vs 16 [5-21]). The cumulative incidence of patients with complications at 180 days was lower in the PPI-24/7 period: 9% vs 17% (adjusted odds ratio, 0.5; P=.002), due to a significant reduction in preimplant complications: 2.5% vs 12% (P <.001). The average number of hospital stays was reduced by 2 per patient in the PPI-24/7 period (nonparametric P <.001). PPI-24/7 implants performed outside working hours (n=178) were safe, with a 180-day cumulative incidence in procedure-related complications of 3.9%.
ConclusionsAmong patients with ASB, PPI-24/7 was associated with a significant reduction in patient morbidity and efficient hospital resource use.
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm