To the Editor:
During exercise stress testing, approximately 0.3% of patients develop transient ventricular conduction defects including left branch block (3 out of 4 cases) (LBBB).1 Of these, 70% occur in patients with documented baseline cardiomyopathy of different etiologies (ischemic heart disease, hypertensive or valvular cardiomyopathy, degenerative disturbances of the conduction system, etc). In patients with normal coronary arteries and without other underlying illness, the association of chest pain and transitory LBBB was first described in 1976 and is known as painful LBBB.2
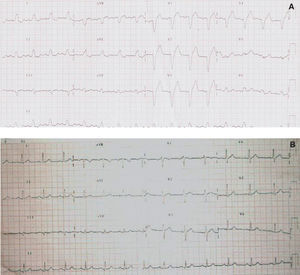
A 57 year-old man, with left nephrectomy for renal neoplasia, with no known cardiovascular risk factors or history of cardiomyopathy, was admitted to our hospital with symptoms of retrosternal pain irradiating to the epigastrium and accompanied by sweating, paleness and tachycardia (105 bpm). Physical examination showed blood pressure 120/70 mm Hg, with no other data of interest. The initial electrocardiogram (ECG) showd LBBB. After administration of sublingual Cafinitrina®, chest pain receded and LBBB disappeared in the ECG, with the trace falling to 65 bpm and normal repolarization. A new episode of chest pain followed the same pattern (Figure A and B). Cardiac enzyme levels were normal in repeated testing. Diagnosed with acute coronary syndrome, cardiac catheterization was performed finding normal left ventricle and absence of lesions in both coronary arteries. The patient was discharged at 48 hours with no other incident and prescribed low molecular weight heparin and a calcium antagonist. At 1 year, she continued asymptomatic with normal ECG and had not presented a similar episode.

Figure. A: left branch block during the episode of pain. B: electrocardiogram after disappearance of precordial pain with disappearance of the left branch block.
The pathophysiology of painful LBBB is unknown. Although some authors have suggested it is caused by microvascular ischemia, basing themselves on finding of high levels of lactate in the coronary sinus,3 the most widely accepted view today attributes it to a dysynergy of the contraction with mechanoreceptor stimulation causing chest pain.4
The interest of this patient lies in our having been able to observe LBBB during episodes of such intense chest pain and accompanied by nausea and vomiting, at rest. The discrete increase in heart rate during pain does not permit us to attribute the conduction disturbance to a frequency-dependent mechanism. Almost all episodes of painful LBBB described previously have been related to increased heart rate during exercise.1-3 In our patient, with angina at rest and angiographically normal coronary arteries without other cardiac illness, a hypothesis of microvascular angina seems most plausible after discounting a heart rate dependent mechanism.
It is difficult to diagnose acute ischemia in patients with LBBB as many ECG diagnostic criteria are not applicable. Anomalous ventricular depolarization produces secondary alteration in the process of recovery, a phenomenon that appears in the ECG with changes in repolarization in a direction opposite to the principal QRS deflection or "appropriate discordance" between the QRS complex and ST-segment. Elevation of ST-segment in association with positive QRS complex, or ST-segment depression in V1, V2 or V3 leads do not occur in uncomplicated bundle branch block, known as "inappropriate discordance," which is indicative of acute ischemia. Extreme ST-segment elevation (>5 mm) in V1 and V2 also indicate acute ischemia. Given the high mortality of myocardial infarction electrically hidden by LBBB,5 the norm should be to perform immediate cardiac catheterization.