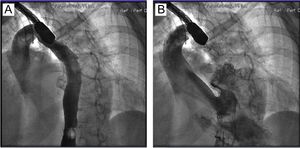
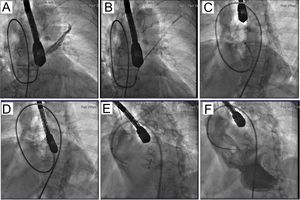
A 78-year-old woman was diagnosed with platypnea-orthodeoxia syndrome caused by patent foramen ovale (PFO) with right-left flow and orthostatic desaturation (78%). PFO closure was scheduled. During the procedure, the inferior vena cava was found to be missing and a large azygos vein was present that drained into the superior vena cava (Figure 1A). The contrast administered entered the left atrium through a tunneled PFO (Figure 1B). This anatomical feature complicated the procedure, and it was necessary to pass a JL4 guide catheter through the PFO and, using this catheter, place a coronary guidewire in the pulmonary vein (Figure 2A). Subsequently, with the help of a daughter catheter, a balloon was placed in the pulmonary vein, thus allowing an anchoring maneuver (Figure 2B). This enabled advancement of the guide catheter followed by introduction of a stiff guidewire into the left atrium, thereby allowing cannula advancement (Figure 2C). An Amplatzer 25mm device was introduced via the cannula, and the first the left disc (Figure 2D) and then the right disc (Figure 2E) were deployed. After full deployment, contrast no longer passed from the left atrium (Figure 2F).


The scientific literature has few reports of PFO closure in the absence of inferior vena cava and, to the best of our knowledge, this is the first case with concurrent platypnea-orthodeoxia syndrome. Closure in such conditions is feasible, although the technique is more difficult. An alternative approach in these cases could be via the jugular or transhepatic vein.