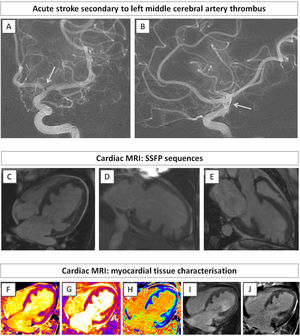
A 34-year old woman with a past medical history of hypertension presented to the emergency department with sudden-onset dysarthria, right facial droop, and right-sided weakness. Her intracranial computed tomography (CT) angiogram confirmed acute stroke, with a thrombus in the left middle cerebral artery (figure 1A,B, white arrow). The patient underwent successful thrombolysis and thrombectomy. Electrocardiogram confirmed sinus rhythm with left bundle branch block. Echocardiogram showed a severely dilated left ventricle with abnormal myocardial architecture and severe systolic impairment. There was no evidence of patent foramen ovale. Her chest X-ray showed pulmonary edema, suggestive of decompensated heart failure.

A cardiac magnetic resonance was conducted to further assess her phenotype. The study showed abnormal myocardial structure, in the spectrum of left ventricular noncompaction, previously described as “saw-tooth cardiomyopathy” (figure 1C-E). There was no inducible ischemia. Tissue characterization analysis showed high-normal myocardial T1 values, in keeping with diffuse myocardial injury (figure 1F), while T2 mapping showed no myocardial edema (figure 1G), with normal extracellular volume (figure 1H). There was no evidence of intracardiac thrombus (figure 1I), although this may indicate previous embolization or successful thrombolysis. On late gadolinium enhancement, there was no myocardial fibrosis or previous infarct (figure 1J). Anticoagulation was commenced, and a resinchronization device was implanted due to left bundle branch block and persistent systolic dysfunction despite optimal medical therapy. The patient provided consent for the publication of her information in this article.
Saw-tooth cardiomyopathy is a rare entity that can present as acute cardioembolic stroke and severe myocardial impairment. The role of cardiac magnetic resonance is crucial in assessing the phenotype and prognosis in these patients.
FUNDINGNone.
AUTHORS’ CONTRIBUTIONSÁ. García-Ropero contributed to the design, writing and imaging preparation of the submitted manuscript. D. Antonakaki contributed to the design and writing of the submitted manuscript. K. Savvatis contributed to the design, writing, and review of the submitted manuscript.
CONFLICTS OF INTERESTNone of the authors have any conflicts of interest to declare.