The Working Group on Cardiac Catheterization and Interventional Cardiology presents a yearly report on the data collected for the national registry. This information shows how procedures are distributed throughout Spain and makes comparisons with other countries feasible.
MethodsInstitutions provided their data voluntarily (online) and were analyzed by the Working Group's Steering Committee.
ResultsData were provided by 108 hospitals (72 public and 36 private) that mainly treat adults, covering 138480 diagnostic procedures, 123746 of which were coronary angiograms, slightly more than the year before, with a rate of 3008 coronary angiograms per million population. Percutaneous coronary interventions decreased slightly to 63202 procedures with a rate of 1373 interventions per million population. Of the 94701 stents implanted, 61% were drug-eluting stents. In the acute phase of myocardial infarction, 15491 coronary interventions were performed, 9.4% more than in 2010, representing 24.6% of the total number of coronary interventions. The most frequent intervention for adult congenital heart disease was atrial septal defect closure (298 procedures). Percutaneous mitral valvuloplasty continued to decrease (286 procedures) and percutaneous aortic valve implantations increased, but at a slower pace than in the previous year, with 770 units implanted in 2011.
ConclusionsThe greatest increase in activity has occurred in the field of myocardial infarction and percutaneous aortic valve implantation. The number of other procedures, both diagnostic and therapeutic, remained stable.
Keywords
Another year has passed and we continue an annual tradition founded in 1990. One of the most important tasks of the Steering Committee of the Working Group on Cardiac Catheterization and Interventional Cardiology is to collect data on the activity of as many cardiac catheterization laboratories as possible to complete the annual registry of activity. In recent years, data collection has steadily improved1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20 due to introducing data online; over the last 2 years, 100% of the hospitals have provided their data. Data cleaning was performed by the steering committee and its members; the preliminary data were presented at the annual meeting of the working group, which this year was held on June 14-15 in Santander (Spain). The data are also available at the working group's website.21
The quality of information obtained provides an overview of the current situation in Spain and makes comparisons with other countries feasible. It also offers a way to assess and compare the development of interventional cardiology in Spanish autonomous communities. The free availability of these data helps in understanding the distribution of resources and in assessing the different trends in the use of diagnostic and therapeutic procedures.
In 2011, the severe economic crisis affecting Europe in general, and Spain in particular, appears to have influenced the evolution of interventional cardiology in the country, clearly limiting the use of resources which, in the case of our specialty, are relatively expensive. In recent years, percutaneous coronary intervention (PCI) has entered a plateau phase with minimal growth; this was negative in 2011 because for the first time the number of angioplasties decreased. However, there has been a continuing increase—already observed in the 2 previous years—of PCI, especially primary angioplasty, in the setting of infarction. There are probably several reasons for this increase, but it may well have been influenced by the European “Stent for Life” initiative,22 which has the aim of improving the treatment of infarction and has named Spain as one of its “target” countries.23 In fact, this year several Spanish regional governments have joined this initiative, which has entailed a significant increase in the number of primary PCI procedures. Finally, the geometric increase in percutaneous aortic valve replacement, both in the number of units implanted and the number of hospitals performing the technique, that was observed in 2010 has undergone a very clear slowdown, probably because of the economic recession.
This article presents the 21st report of interventional activity in Spain, covering the activity of all public hospitals and a significant number of private hospitals.
MethodsWe collected data on diagnostic and interventional cardiovascular procedures performed in most Spanish hospitals. Institutions provided their data on a voluntary basis without audit. Anomalous data or data with values outside trends in a given hospital in recent years were referred back to the researcher responsible for the hospital for their reassessment. Data were collected using a standard electronic questionnaire, which was accessed through the website of the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology and completed online.21 With the collaboration of the Persei company, the steering committee of the working group analyzed the data obtained, which are presented in this article, although a preliminary outline was presented as a slideshow at the working group's annual meeting.
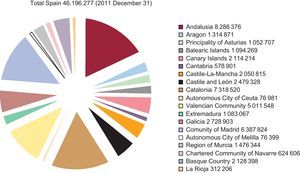
Population-based calculations for Spain and each autonomous community were based on the size of the population estimated by the Spanish National Institute of Statistics up to December 31, 2011, as published on its website.24 The Spanish population was estimated at 46196277 inhabitants (Figure 1). As in 2010, the procedures per million population for the entire country were based on the total population, because in previous years these rates were calculated based on averages from the different provinces in which interventional cardiology was conducted, rather than on the total population: although the differences may be small compared to previous years, the final result is closer to reality.

Figure 1. Population of Spain as of 31 December, 2011. Source: Spanish National Institute of Statistics.
As in previous registries, a hospital was considered to be public that, regardless of its source of funding, had contracted to serve a specific area of the population within the public health system. Other hospitals were considered to be private.
Results Infrastructure and ResourcesA total of 108 hospitals performing interventional procedures in adults participated in the present registry (5 fewer than the previous year); of these, 12 (2 more than in 2010) hospitals performed these procedures in pediatric patients (Appendix). All the public hospitals (72) and 36 of 110 private hospitals submitted their data, representing almost all the hospitals performing interventional procedures in Spain. There were 171 cardiac catheterization laboratories, of which 126 (74%) were in public hospitals; 35 hospitals had 2 laboratories and 7 had 3 or more. A 24-h emergency team was available in 69% of the hospitals and 63% performed cardiac surgery.
Regarding personnel, the 108 hospitals reported 438 physicians (339 of whom were accredited) who performed interventional procedures in 2011. There were 2.64 physicians per laboratory in public hospitals (333 physicians) and 2.33 per laboratory in private hospitals. There were 530 registered nurses and 93 radiology technicians, with a combined average of 3.90 per public hospital and 2.93 per private hospital.
Diagnostic ProceduresDuring 2011, 138480 diagnostic procedures were performed, representing a 2.2% increase compared to the previous year. In total, 123746 coronary angiograms were performed, which was 3.8% more than in 2010. Of these procedures, 23.5% were performed in women and 23.3% in patients over 75 years; these figures remain very stable from year to year. The national average was 3008 coronary angiograms per million population, which was higher than previous years. Compared to the 19.6% increase in the number of valvular procedures observed in 2010, this year there has been a 9% decrease.
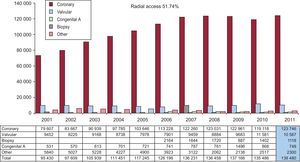
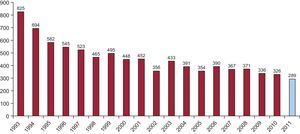
Figure 2 shows the distribution of all diagnostic procedures performed since 2001.

Figure 2. Evolution of the number and type of diagnostic procedures performed between 2001 and 2011.
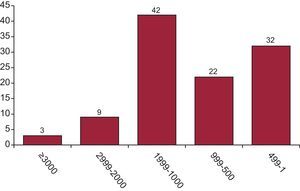
Regarding diagnostic activity, 54 hospitals performed more than 1000 coronary angiograms (8 fewer than in 2010), of which only 12 performed more than 2000 (9 fewer hospitals than in the previous year) (Figure 3). There was an average of 1282 diagnostic procedures per hospital, which was virtually the same as in previous registries.18, 20 Of note, only 19 public hospitals (6 more than in 2010) performed fewer than 1000 coronary angiograms.

Figure 3. Distribution of hospitals according to the number of coronary angiograms.
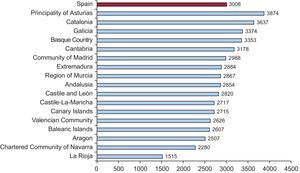
Figure 4 shows the national average of 3008 coronary angiograms per million population. Compared to the previous year, the difference (2359 procedures) between the region performing the most coronary angiograms and the region performing the fewest has increased. If we exclude the two most extreme values, the sample is much more homogeneous, with a difference of only 1130 procedures.

Figure 4. Distribution of coronary angiograms per million population and autonomous communities.
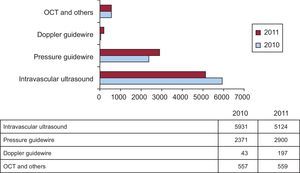
Regarding intracoronary diagnostic techniques, for the first time there was a clear and significant decrease of 14% in the use of intravascular ultrasound, although it remains the most widely used technique. The use of pressure guidewire continued to steadily increase; last year the increase was 26.6%, whereas this year it was 22%, totaling 65% growth in the last 3 years. The use of optical coherence tomography remained exactly the same as last year. Figure 5 shows the evolution of the different intracoronary diagnostic techniques compared to last year.

Figure 5. Evolution of the different intracoronary diagnostic techniques. OCT, optical coherence tomography.
Regarding access routes, the radial artery was used in 51.7% of cases, a figure similar to previous years, although this was 5% less than in 2010.
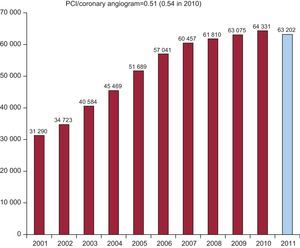
Percutaneous Coronary InterventionFor the first time, there was a reduction in the number of PCI: 63202 procedures were performed, 1129 less than in 2010, representing a 1.8% decrease. Figure 6 shows the historical development of PCI. The number of PCI per million population was 1373 which, compared to 1398 in 2010, represented a 1.8% decrease. All the hospitals that performed diagnostic procedures also performed PCI.

Figure 6. Evolution of the number of percutaneous coronary interventions performed between 2001 and 2011. PCI, percutaneous coronary intervention.
The ratio of PCIs to coronary angiographies was around 0.51 (0.54 in 2012). The number of procedures for multivessel disease remained very stable compared to the previous year, representing 25.8% of all PCIs; there was very little change (a 3% decrease) in the number of ad hoc procedures performed during diagnosis (74%).
The distribution by sex and age remained very similar to 2010, with 21.5% of PCIs performed in women and 24.7% in those over 75 years. Restenosis was treated by PCI in 5% of cases (5.3% in 2010).
Strikingly, there was a marked decrease in procedures involving the unprotected left main coronary artery; there were 1828 interventions, 20% fewer than the previous year (a return to the same levels as in 2008), representing 2.9% of total PCI. Use of PCI for unprotected left main coronary artery disease is discussed in the “Discussion” section. There were 952 and 153 interventions on the saphenous vein and mammary artery, respectively, which in both cases was fewer than in previous registries.
Glycoprotein IIb/IIIa inhibitors and adjunctive antithrombotic drug therapy were used in 11081 procedures, representing 17.5% of PCI (4% less than the previous year): 64% were performed using abciximab, 8% with tirofiban, 3% with eptifibatide, and 25% with bivalirudin; the use of bivalirudin continues to increase over previous years.
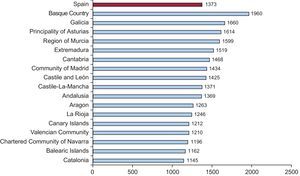
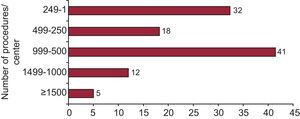
Figure 7 shows the distribution by Spanish autonomous communities of the 1373 PCIs per million population. The size of the difference (815) was maintained between 2009 and 2010, although if the 2 extremes are eliminated, the figure becomes more homogenous at 498. Regarding distribution per hospital (Figure 8), 50 hospitals performed fewer than 500 PCIs per year (46%), with most of the private hospitals being in this category. As in 2009 and 2010, there were 17 hospitals in the high-volume (>1000) category.

Figure 7. Distribution of percutaneous coronary interventions per million population and autonomous communities.

Figure 8. Distribution of hospitals according to the number of percutaneous coronary interventions performed in 2011.
There was a clear difference in the use of intracoronary diagnostic techniques (intravascular ultrasound and pressure guidewire), which are mainly used to evaluate the severity of intermediate lesions or the results of intervention. The use of intravascular ultrasound decreased to 8.1% of interventions (1.1% less than in 2010), whereas there was a clear rise in the use of pressure guidewire to 4.6% of interventions (compared to 3.7% in 2010 and 2.5% in 2008).
Radial access in PCI grew by 7% to reach 55.5%, for the first time exceeding femoral access in PCI. Vascular closure procedures continued to decrease, with a total of 35330 cases, almost 2000 fewer than the previous year. Collagen was used in 63% of the procedures, suture in 13%, and other devices in 24%.
StentsStents were implanted in 89% of all PCIs (5% less than in 2010), with 94701 units implanted during 56078 PCIs in 2011; this represented 7000 fewer units than in 2010 and more than 10000 fewer than in 2009. Once again, the ratio of stents per patient decreased to 1.5 (1.56 in 2010 and 1.63 in 2009). The use of drug-eluting stents remained completely stable at 61%, representing 58211 units. Whether one type of stent or both were used depended on the characteristics of the patient and the target lesions; specifically, the percentage of procedures using drug-eluting stents alone was 35%, similar to 2009 and 2010, but almost 20% less than in 2008.
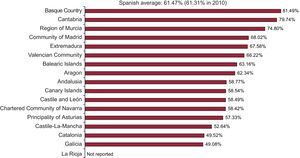
The use of drug-eluting stents continued to vary significantly between the Spanish regions. This year, more were used in the Basque Country (81.5%) then in Cantabria (79.7%), whereas the fewest (49%) were used in Galicia (Figure 9).

Figure 9. Distribution of antiproliferative drug-eluting stents as a percentage of all stents implanted per autonomous communities.
Other Devices and Percutaneous Coronary Intervention ProceduresThe rate of increase in the use of rotational atherectomy slowed, with 1225 procedures compared to 1213 in the previous year. The use of directional atherectomy or intracoronary brachytherapy was not reported. Among other devices, the use of cutting balloons fell for the first time in recent years, being used in 1916 procedures in 2011 compared to 2092 procedures in 2010, a decrease of 9%. The spectacular growth in the use of thrombectomy catheters continued, with 8171 procedures in 2011, which was 16% more than in 2010 and almost 50% more than in 2009.
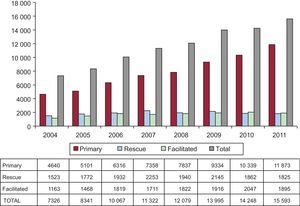
Intervention in Acute Myocardial InfarctionThe 15593 PCIs performed in the setting of acute myocardial infarction (AMI) represents a 9.4% increase compared to 2010, which was 6% higher than in 2009, and now represents 24.6% of all PCIs. Of the total number of procedures, 18.5% were performed in women and 20.7% in patients older than 75 years.
Within the range of PCI procedures in the acute phase of AMI, primary angioplasty continued to increase, the only approach to do so, increasing from 9334 in 2009 to 10339 in 2012 and to 11766 in 2011. In 2010, the Principality of Asturias, Castile-La-Mancha, Catalonia and the Region of Murcia led growth in the number of procedures, whereas this year the leading regions were the Principality of Asturias, the Valencian Community, Castile-La-Mancha, Castile and León, Andalusia and Aragon. Primary PCI accounted for 18.6% of all angioplasties and 76% of all infarct PCIs; the number of both facilitated PCIs and rescue PCIs slightly decreased (Figure 10).

Figure 10. Evolution of the types of percutaneous coronary intervention in acute myocardial infarction.
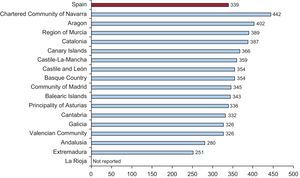
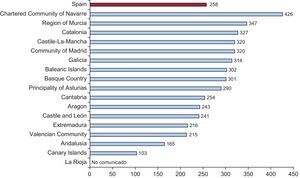
The national distribution of PCI in AMI was similar to that of previous years; the best data were provided by those regions that had instituted a continuous care program for AMI (Figure 11, Figure 12).

Figure 11. Distribution of percutaneous coronary interventions in acute myocardial infarction per million population and autonomous communities.

Figure 12. Distribution of primary angioplasties per million population and autonomous communities.
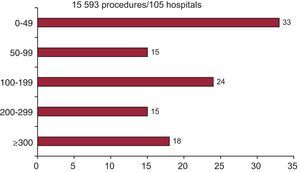
Regarding the number of procedures per center, 33 performed more than 200 infarct PCI per year (6 more than in 2010), whereas 33 performed less than 50 (7 less than the previous year) (Figure 13).

Figure 13. Distribution of hospitals according to the number of percutaneous coronary interventions acute myocardial infarction.
Noncoronary Interventions in AdultsMitral valvulopasty remained the most frequent valvuloplasty (289 cases), although the steady yearly decrease in its use continued. The technique was performed in 54 of the 108 centers (Figure 14). Aortic valvuloplasty continued to increase, albeit at a slower pace, with 173 procedures in 2011 compared to 146 in 2010. The growth in transcatheter aortic valve implantation continued, although more moderately, increasing from 426 in 2009 to 655 in 2010 and 770 in 2011 (48 hospitals performed the technique, 9 more than in 2010). Of these, 53% of the devices were self-expanding (92.7% were successful; hospital mortality was 5.3%) and 47% were balloon-expandable devices (92.7% were successful; hospital mortality was 5.3%).

Figure 14. Evolution of mitral valvuloplasty in Spain.
The treatment of adult congenital heart disease remained the most frequent noncoronary intervention procedure, although the number of such procedures sharply decreased. In total, 565 procedures were performed (compared to 682 in 2010); the most common procedure was atrial septal defect closure (298 procedures; 97% were successful). There were major complications in 1.5% and another 1.5% were classified as failures without complications. Foramen ovale closure was performed in 195 cases (265 in 2010); 97% were successful and there was only 1 major complication. In total, 32 procedures for aortic coarctation were performed (15 fewer than the previous year). Other procedures included the closure of ductus, ventricular septal defects, and fistulas. A total of 126 paravalvular leaks were treated, 12 more than in 2010.
Interventions in Pediatric PatientsTwelve hospitals provided data on their activity in pediatric patients (aged≤16 years), involving 48 septal closures and 92 ductus closures as the most common procedures.
DiscussionThe data collected on 2011 activity shows a trend towards the leveling out or a slight decrease in both diagnostic and interventional activity, and only shows an increase in newer techniques, such as percutaneous aortic valve implantation, although this increase was less than in the previous year.
It should be noted that the data for this year's and last year's registries were collected online alone. Despite this, there was no reduction in the number of participating hospitals, particularly if we focus on public hospitals, which account for the bulk of the activity. Furthermore, the provision of human and material resources remained very stable in recent years, with the vast majority of interventional cardiologists being accredited (77%).
Diagnostic procedures increased slightly from 2945 coronary angiograms per million population to 3008. This is still well below the latest published figures for Europe for 2005, with an estimated 4030 coronary angiograms per million population25 or the latest data referring to 2009 presented at the EuroPCR 2011 congress, which reported an average of more than 5500 coronary angiograms per million population.26 A striking fact is that the number of high-volume hospitals has slightly decreased, since 6 hospitals that performed more than 1000 coronary angiograms in 2010 have not done so this year; in fact, 19 public hospitals were recorded as performing fewer than 1000 coronary angiograms per year.
Regarding interventional procedures, for the first time there has been a decrease in the number of PCIs to around 63202 procedures, which is more than 1000 fewer than the previous year. The decrease seems to have a multifactorial explanation. On the one hand, there has been no increase in diagnostic procedures, thus making an increase in interventionist procedures unlikely. On the other hand, it currently appears that some “complex” cases are not treated percutaneously, since there have been decreases in the number of stents implanted, the stent/patient ratio, and the number of special devices, such as rotational atherectomy or cutting balloon, used in these types of cases. In addition, there has been a marked increase in use of the pressure guidewire; as mentioned in the FAME study,27 this tends to reduce the number of PCI procedures and the number of stents used. Finally, the long-term results of the SYNTAX trial28 may also be contributing to the increase in the number of complex cases referred to bypass surgery. In this sense, the sharp decrease in the case of percutaneous treatment of the unprotected left main coronary artery is especially noteworthy. As a final note on PCI, we would like to draw attention to how different the situation is in Spain compared to the rest of Europe: the figure of 1373 PCI procedures per million population in Spain is well below the latest European figure of 1601 PCI procedures per million population in 200525 or the nearly 2000 per million population in 2009.26
Among the most promising data in recent years, especially this year, is the improvement in the number of primary PCIs, which is clearly related to the implementation of the “Stent for Life” initiative of the European Society of Cardiology.22 In fact, the recent article by Kristensen et al.29 cites Spain as one of the countries with the best response to the initiative. Growth in primary PCI was 13.8%−and more than 20% in the last 2 years−whereas rescue or facilitated angioplasty slightly decreased. In fact, the increase in primary PCI is the reason the total number of PCIs has not changed very much. In addition, the increase in primary PCI explains the increased use of thrombectomy catheters and may also explain, at least partly, the decrease in the stent/patient ratio, since these procedures typically involve the use of just one stent. Although the situation has improved, we are still far from reaching the target of a “Stent for Life.” Despite there being no data on the total number of AMI with ST-segment elevation cases in Spain, if the annual estimate was 45000 AMI in Spain,30, 31 then primary PCI would be performed in only 20%; the aim of the “Stent for Life” initiative is to achieve primary PCI in 70% of AMI.22
Another encouraging fact is that percutaneous aortic valve implantation increased by 17.5%, although this represents a slowdown compared to the previous year, when the increase was 54%. The economic crisis could be having a strong impact on this area due to the high price of the devices. However, once the economic situation improves, together with probable reductions in the price of the devices due to the arrival of new competitors, the number of procedures in this area should begin to increase again in the future.
ConclusionsIn the 2011 data we have seen a continuation of the leveling out or a slight decrease in the evolution of diagnostic and therapeutic procedures. Angioplasty procedures in the context of AMI continue to increase, especially primary PCI, due to the incorporation of new regions into primary PCI programs and to the marked increase in primary PCI in some hospitals. The “Stent for Life” program, which is a priority for the European Society of Cardiology, the Spanish Society of Cardiology, and our own working group, appears to be raising awareness among policy makers and medical professionals regarding the need to improve myocardial infarction care in Spain as a means to improve both the length and quality of life of coronary patients.
Differences remain between regions in the use of PCI in general and infarct PCI in particular.
Special mention must be made of percutaneous aortic valve implantation; despite a 17.5% increase in the number of procedures, growth was slower compared to the previous year.
Conflicts of interestNone declared.
Acknowledgements
The Board of the Working Group on Cardiac Catheterization and Interventional Cardiology would like to thank the directors and staff of Spain's catheterization laboratories, as well as those responsible for data collection, for all their work which made this registry possible.
Appendix. Hospitals participating in the 2011 registry| Public hospitals | Private hospitals |
| Andalusia | |
| Complejo Hospitalario Torrecárdenas | Clínica Nuestra Señora de la Salud |
| Complejo Hospitalario Universitario de Jaén | Clínica Santa Elena, Estepona |
| Complejo Universitario Carlos Haya | Hospiten Estepona |
| Hospital Clínico Universitario Virgen de la Victoria | |
| Hospital Costa del Sol | |
| Hospital de Jerez de la Frontera | |
| Hospital Juan Ramón Jiménez | |
| Hospital Universitario de Valme | |
| Hospital Universitario Puerta del Mar | |
| Hospital Universitario Puerto Real | |
| Hospital Universitario Reina Sofía | |
| Hospital Universitario Virgen de las Nieves | |
| Hospital Universitario Virgen del Rocío | |
| Hospital Universitario Virgen Macarena | |
| Aragon | |
| Hospital Clínico Universitario Lozano Blesa | |
| Hospital Universitario Miguel Servet | |
| Principality of Asturias | |
| Hospital Central de Asturias | Centro Médico de Asturias |
| Hospital de Cabueñes | |
| Cantabria | |
| Hospital Universitario Marqués de Valdecilla | |
| Castile and León | |
| Hospital Clínico Universitario de Salamanca | Hospital Campo Grande (CEMIN) |
| Hospital Clínico Universitario de Valladolid | |
| Hospital de León | |
| Hospital General Yagüe | |
| Castile-La-Mancha | |
| Hospital General de Ciudad Real | |
| Hospital General Universitario de Albacete | |
| Hospital General Universitario de Guadalajara | |
| Hospital Virgen de la Salud | |
| Catalonia | |
| Ciutat Sanitària i Universitària de Bellvitge | Centre Cardiovascular Sant Jordi |
| Hospital Clínic i Provincial de Barcelona | Hospital General de Catalunya |
| Hospital de la Santa Creu i Sant Pau | Hospital Quirón Barcelona |
| Hospital del Mar | Hospital Universitari Mútua de Terrassa |
| Hospital General Universitari Vall d’Hebron | |
| Hospital Universitari Dr. Josep Trueta | |
| Hospital Universitari Germans Trias i Pujol | |
| Hospital Universitari Joan XXIII | |
| Hospital Universitario Arnau de Vilanova | |
| Valencian Community | |
| Hospital Clínico Universitario de Valencia | Clínica Medimar, Alicante |
| Hospital de la Ribera, Alzira | Hospital Clínica Benidorm |
| Hospital General de Alicante | Hospital del Vinalopó |
| Hospital General de Castellón | Hospital IMED Levante |
| Hospital General Universitario de Elche | Hospital Perpetuo Socorro de Alicante |
| Hospital General Universitario de Valencia | Hospital San Jaime Torrevieja USP |
| Hospital Universitario Dr. Peset | UTE Torrevieja Salud |
| Hospital Universitario La Fe | |
| Hospital Universitario San Juan de Alicante | |
| Extremadura | |
| Hospital de Cáceres | |
| Hospital Universitario Infanta Cristina | |
| Galicia | |
| Complexo Hospitalario Universitario A Coruña | Instituto Médico Quirúrgico San Rafael |
| Complexo Hospitalario Universitario de Santiago | |
| Complexo Hospitalario Universitario de Vigo | |
| Balearic Islands | |
| Hospital Universitario Son Dureta | Clínica Juaneda |
| Clínica Rotger | |
| Clínica USP Palmaplanas | |
| Policlínica Miramar | |
| Canary Islands | |
| Hospital de Gran Canaria Dr. Negrín | |
| Hospital Universitario de Canarias, Tenerife | |
| Hospital Universitario Insular de Gran Canaria | |
| Hospital Universitario Nuestra Señora de Candelaria | |
| Hospiten Rambla | |
| Community of Madrid | |
| Hospital Central de la Defensa Gómez Ulla | Clínica Nuestra Señora de América |
| Hospital Clínico San Carlos | Clínica Ruber |
| Hospital de Torrejón | Fundación Jiménez Díaz |
| Hospital General Universitario Gregorio Marañón | Hospital La Moraleja (SANITAS) |
| Hospital Puerta de Hierro | Hospital La Zarzuela |
| Hospital Ramón y Cajal | Hospital Universitario Quirón Madrid |
| Hospital Universitario 12 de Octubre | Hospital de Madrid Norte Sanchinarro |
| Hospital Universitario de la Princesa | Sanatorio del Rosario de Madrid |
| Hospital Universitario Fundación Alcorcón | Sanatorio La Milagrosa |
| Hospital Universitario La Paz | |
| Region of Murcia | |
| Hospital Universitario Santa María del Rosell | Hospital San Carlos, Murcia |
| Hospital Universitario Virgen de la Arrixaca | Hospital Virgen de la Vega |
| Chartered Community of Navarre | |
| Hospital de Navarra | |
| Basque Country | |
| Hospital de Basurto-Basurtuko Ospitalea | Clínica Vicente San Sebastián |
| Hospital de Cruces | Policlínica Guipúzcoa |
| Hospital de Galdakao-Usansolo | |
| Hospital Txagorritxu | |
| La Rioja | |
| Hospital Viamed-Los Manzanos |
Corresponding author: Unidad de Hemodinámica, Hospital Juan Ramón Jiménez, Ronda Norte s/n, 21005 Huelva, Spain. jfdiazf@yahoo.es