Keywords
INTRODUCTION
This article reports the findings from the 2009 Spanish Catheter Ablation Registry. The registry is run by the Spanish Society of Cardiology Working Group on Electrophysiology and Arrhythmias and this is the ninth consecutive year that the findings have been published.1-8 The Registry covers the whole of Spain and data are collected annually. Participation is voluntary, although most of the arrhythmia units in Spain collaborate. This makes it one of very few existing large-scale observational records of catheter ablations.
The Registry's objectives are primarily to observe and describe the changes in the interventional treatment of cardiac arrhythmias in Spain, and to provide reliable information about the activities carried out and the resources available in arrhythmia units.
METHODS
As in previous years, data were collected either, prospectively or retrospectively. In the prospective approach, individual patients were included in a standard database provided by the Registry. In the retrospective approach, a standard questionnaire was sent to all interventional electrophysiology laboratories in January 2010. The questionnaire was also available on the website of the Electrophysiology and Arrhythmias Working Group (www.arritmias. org). All data collected were treated anonymously. Even the Registry coordinators were unaware of the origin of the data, as the Spanish Society of Cardiology secretariat ensured that participating centers could not be identified.
Information on the technical and human resources available in each participating arrhythmia unit was collected, together with data on procedures performed and patient demographic characteristics. As in previous years, data on human resources were only collected for public hospitals, and epidemiological data are only presented for centers with prospective data collection.
We analyzed the same 10 arrhythmia substrates collected in previous registries: atrioventricular nodal reentrant tachycardia (ANRT), accessory pathway (AP), atrioventricular node (AVN), focal atrial tachycardia (FAT), cavotricuspid isthmus (CTI), macroreentrant atrial tachycardia (MAT), atrial fibrillation (AF), idiopathic ventricular tachycardia (IVT), ventricular tachycardia with postinfarction scar (VT-AMI), and ventricular tachycardia associated with nonischemic heart disease (VTNAMI). We analyzed several variables which were common to all substrates, including the number of patients and procedures performed, the success rate, type of ablation catheter used, and the number and type of complications reported in connection with the procedure, including periprocedural death. We also collected a number of variables which were specific to particular substrates, such as the anatomical location of accessory pathways, the location and mechanism of atrial tachycardias, and the type of ventricular tachycardia.
As in previous years, the success rate refers only to status on completion of the procedure (acute success rate). It was not possible to calculate the rate of recurrence because long-term follow-up was not available. Several therapeutic approaches with differing objectives exist for AF and VT-AMI substrates, so criteria for success or failure may differ depending on the technique used. For this reason, when the overall success of the ablation procedure was analyzed, AF and VT-AMI were excluded. Only complications reported during the post-procedure hospital stay were recorded.
Statistical Analysis
Quantitative variables were expressed as means (SD). Differences between quantitative variables were assessed using Student t test for dependent or independent samples, as appropriate. The c2 and Fisher exact tests were used to analyze differences between categorical variables. Statistical significance was established at P<.05. Statistical analysis was performed using the SPSS 15.0 statistics package.
RESULTS
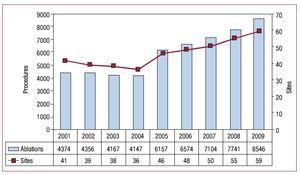
In total, 59 sites submitted data this year (Figure 1), and so once again the number of sites participating in the Registry increased. Of the participating sites, 49 (83%) belong to the public health system and 10 (17%) are private institutions.

Figure 1. Change in the number of centers participating and procedures recorded in the Spanish Catheter Ablation Registry
The retrospective data collection method was preferred by most centers, with only 8 centers (13.9%) submitting prospective data.
The characteristics of the participating sites were very similar to previous years. Of note was that most were tertiary hospitals (71%) and cardiology was the department that reported the data in 98% of the cases. University hospitals accounted for 78% of the sample and 80% offered cardiac surgery (Table 1).

Epidemiological Characteristics
As in past registries, patient epidemiological characteristics were only analyzed for data collected prospectively. This year, 8 centers used this method, corresponding to a total of 1344 patients.
The mean age of the patients was 45 (12) years. The youngest patients were those with an AP (36 [10] years) and the oldest were those who underwent AVN ablation (71 [15] years). With regard to distribution of substrates by sex, ANRT ablation was performed primarily in women (77%), whereas AF ablation and treatment of ventricular tachycardias (whether or not associated with structural heart disease) were mainly performed in men (78% and 71%, respectively). As shown, these data are virtually identical to those from the previous registry.
Likewise, 26% of patients had a history of structural heart disease and left ventricular dysfunction was limited to patients undergoing AVN ablation and ventricular tachycardia associated with heart disease. The same distribution was observed for patients who received an implantable cardioverter defibrillator.
Infrastructure and Resources
Tables 1 and 2 detail the technical and human resources available in the laboratories participating in the Registry, as well as their activities. One site was dedicated exclusively to pediatric patients.

A total of 45 sites (76%) had at least one dedicated electrophysiology laboratory. The mean number of days per week that the laboratory was available was 3.6 (1.5) (median, 4). Six centers (10%) had 2 dedicated electrophysiology laboratories.
Defibrillators and pacemakers were implanted in 70% of the laboratories, defibrillators only in 5%, and pacemakers only in 1%. External electric cardioversion was performed in 36 laboratories (61%) and internal cardioversion in 9.
Digital polygraphy was available in 97% of the sites while 71% had digital radiology; 49% of the laboratories had a portable fluoroscope. In 47 centers (80%), a nonfluoroscopic navigation system (NFNS) was available, and 16 and 3 centers had 2 and 3 NFNSs, respectively. An NFNS was available in 86% of the sites in the public health system.
There were still 3 sites with a magnetic navigation system available and there was one site with a robotic navigation system. Laboratories with intracardiac echocardiography constituted 29%. Cryoablation constituted performed in 19 centers (32%)
The number of health care staff in electrophysiology laboratories remained largely unchanged, with 81% of centers having more than 1 full-time physician and 18 (31%) having more than 2 full-time physicians. In total, 88% of the laboratories had at least 2 full-time university nursing graduates. In the 30 public hospitals with student fellowships for catheterization, the mean number per site was 1.3.
Overall Results
This year saw the highest number of ablation procedures recorded in the Registry's history, with a total of 8546 procedures reported by the 59 participating centers (Figures 1 and 2). This represents a mean of 145 (101) ablations per center (median, 133; range, 9-497) .

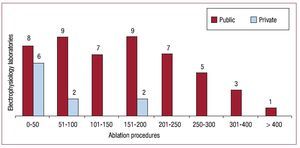
Figure. 2. Number of electrophysiology laboratories in the Spanish Registry by number of ablation procedures performed during 2009.
If we exclude AF and VT-AMI, the overall success rate was 93% (6599/7118). A total of 160 complications (1.9%) was reported for all ablation procedures (including AF and VT-AMI). Four deaths were reported (0.046%); 1 in an ablation of AF, 1 in an ablation procure for an AP, and 2 in a procedure for CTI ablation. Two cases of pulmonary embolism were reported, one during a procedure for AP and the other for FAT. There was one case of ablation catheter entrapment in the mitral valve during ablation of AF. Surgical extraction was required. Eleven cases of iatrogenic AVN block requiring implantation of a definitive pacemakers were reported (0.13%). All these events occurred during ANRT ablation, except for one that occurred during CTI ablation.
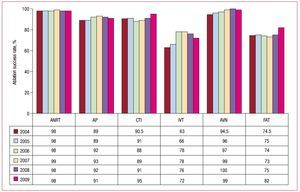
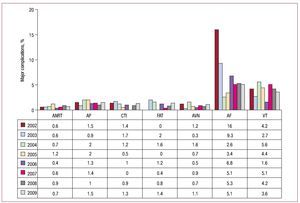
The overall outcomes, both in terms of success rates and complication rates, are compared with previous years in Figures 3 and 4.

Figure 3. Change in catheter ablation success rates since 2004, by substrate treated. Abbreviations: ANRT, atrioventricular nodal reentrant tachycardia; AP, accessory pathways; AT, atrial tachycardia; AVN, atrioventricular node; CTI, cavotricuspid isthmus; IVT, idiopathic ventricular tachycardia.

Figure 4. Percentage of major complications of catheter ablation since 2002, by substrate treated. Abbreviations: AF, atrial fibrillation; ANRT, atrioventricular nodal reentrant tachycardia; AP, accessory pathways; AVN, atrioventricular node; CTI, cavotricuspid isthmus; FAT, focal atrial tachycardia; VT, ventricular tachycardia.
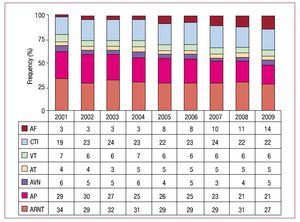
In terms of the frequency of conditions treated, ANRT was still the most common with ablation of CTI the second most common procedure, ahead of AP (Figure 5). The number of AF ablation procedures increased 44% with respect to the previous year and accounted for 14% of the total procedures performed. The change in the relative frequency of different substrates from 2001 is shown in Figure 6.

Figure 5. FRelative frequency of different substrates treated by catheter ablation in Spain during 2009. For each substrate, the percent change from the previous registry is shown. Abbreviations: AF, atrial fibrillation; ANRT, atrioventricular nodal reentrant tachycardia; AP, accessory pathways; AVN, atrioventricular node; CTI, cavotricuspid isthmus; FAT, focal atrial tachycardia; IVT, idiopathic ventricular tachycardia; MAT, macroreentrant atrial tachycardia/atypical atrial flutter; VT-AMI, ventricular tachycardia with postinfarction scarring; VT-NAMI, ventricular tachycardia associated with non-ischemic heart disease.

Figure 6. Change in the relative frequency of the different substrates treated since 2001. Abbreviations: AF, atrial fibrillation; ANRT, atrioventricular nodal reentrant tachycardia; AP, accessory pathways; AT, atrial tachycardia; AVN, atrioventricular node; CTI, cavotricuspid isthmus; VT, ventricular tachycardia.
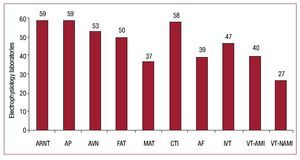
ANRT and AP ablations were performed at all sites and only one public hospital did not perform CTI ablation (Figure 7). As in the previous year, the substrate treated by the fewest sites was VT-NAMI (46%). The proportion of centers performing AF ablation continued to increase and this procedure was performed in 66% of all centers (n=39) and in 71% of public hospitals.

Figure 7. Number of electrophysiology laboratories in the National Registry treating each of the different substrates. Abbreviations: A, atrial fibrillation; ANRT, atrioventricular nodal reentrant tachycardia; AP, accessory pathways; AVN, atrioventricular node; CTI, cavotricuspid isthmus; FAT, focal atrial tachycardia; IVT, idiopathic ventricular tachycardia; MAT, macroreentrant atrial tachycardia; VT-AMI, ventricular tachycardia with postinfarction scar; VTNAMI, ventricular tachycardia associated with nonischemic heart disease.
Atrioventricular Nodal Reentrant Tachycardia
This substrate was addressed in all centers. A total of 2341 ANRT ablation procedures was performed, accounting for 27.4% of all procedures. The mean number of procedures per center was 40 (25) (range, 2-131). The success rate was 98% (2294/2341); 29 centers (49%) achieved a 100% success rate. There were 17 cases of major complications (0.73%): 10 cases (0.43%) of AVN block requiring a permanent pacemaker, 5 cases of vascular access complications, and 2 cases of pericardial effusion that did not require drainage.
The most widely used ablation catheter was the conventional type (radiofrequency catheter with a 4-mm tip). A nonconventional catheter was used in 100 cases (4.3%), specifically in 59 cryoablation catheters, 35 irrigated tip catheters, and 6 catheters with an 8-mm tip.
Cavotricuspid Isthmus
CTI ablation remained the second most common procedure after ANRT ablation. In total, 1859 CTI ablations were performed, giving a mean per center of 32 (23). The procedure was successful in 1760 cases (94.7%). Only 1 center did not perform this type of ablation in 2009, and 25 centers reported 100% success rates. There were 20 major complications (1.1%): 11 vascular complications, 1 case of AVN block that required implantation of a permanent pacemaker, 3 cases of pericardial effusion, 2 cerebrovascular accidents, 2 cases of heart failure, and 2 deaths. One of the deaths occurred in the postoperative period due to a vascular complication.
The use of the 4-mm ablation catheter was the exception with this substrate (2%). The 8-mm catheters were used 914 times, irrigated tip catheters 897 times, and cryoblation catheters 7 times.
Accessory Pathways
In total, 1758 AP ablations were performed, giving a mean per center of 30 (20) (range, 1-77). The procedures were successful in 1607 (91.4%). Of the 46 centers that performed more than 10 such procedures in 2009, only 5 reported 100% success. There were 27 (1.5%) major complications: 15 vascular complications, 8 pericardial effusions (2 with cardiac tamponade), 2 cerebrovascular accidents, 1 pulmonary thromboembolism, and 1 death. The patient who died was 91 years old; the cause of death was not reported. This year, as previously, there were no reports of AVN block during AP ablation.
A conventional catheter was not used in 195 cases (11.1%). Irrigated tip catheters were used 106 times, cryoblation catheters 70 times, and 8-mm catheters 17 times.
The site of the ablated AP was reported in 1696 cases (96.5%). As in previous registries, the most common sites were the left ventricular free wall (52%) and the inferior paraseptal pathway (25%). The site that was ablated least often was the peri-Hisian/superior paraseptal pathway (9%). The success of the ablation procedure depended on the location of the AP: the success rate was 92% (816/884) for ablations in the left free wall, 91% (386/424) in the inferior paraseptal pathway, 89% (212/237) in the right free wall, and 82% (124/151) in the peri-Hisian or superior paraseptal pathways.
Atrioventricular Node Ablation
The total number of AVN ablation procedures performed was 387, and success was achieved in 98.5% of the cases. Five complications (1.3%) were reported: 2 in the vascular access, 2 episodes of congestive heart failure, and 1 pericardial effusion. A conventional catheter was not used in 69 cases: 8 mm catheters were used 41 times, irrigated tip catheters 17 times, the cryoblation catheters 11 times.
Focal Atrial Tachycardia
A total of 283 FAT ablation procedures was performed, with a success rate of 82% (232/283). The intervention was performed in the right atrium in 46 centers, and in the left atrium in only 28 centers. The origin of the FAT was reported in 249 cases; success rates were slightly higher for those arrhythmias originating in the right atrium: 79% (139/176) compared to 75% in the left atrium (55/73).
Four complications (1.4%) were reported: 3 pericardial effusions, 2 of which were associated with cardiac tamponade, and 1 case of pulmonary embolism.
A special catheter was used in 65 cases: 8 mm catheters were used 8 times, cryoblation catheters 2 times, and irrigated-tip catheters 55 times.
Macroreentrant Atrial Tachycardia/Atypical Atrial Flutter
This substrate was addressed in 37 centers (63%), with a total of 201 procedures (mean, 5.4 [range, 1-25] procedures per center). The procedure was successful in 141 cases (70.1%). Eight complications (4%) were reported: 2 cerebrovascular accidents, 3 femoral vacular complications, and 3 cardiac tamponades.
In 184 procedures, information on the origin of the MAT was available: 88 procedures were performed in the right atrium compared to 96 in left atrium, with success rates of 76% and 62%, respectively. In 70% of procedures, a catheter tip other than 4 mm was used; in most of these cases, an irrigated tip catheter was used (85%).
Atrial Fibrillation
A total of 1188 AF ablation procedures was performed in 39 centers (66%). This represents a mean of 30 (range, 2-129) procedures per center, although 16 laboratories performed fewer than 15 procedures. Nine centers performed more than 50 and 3 performed more than 100.
The technical approach was reported in 1094 of these procedures (92%). Ostial electrical disconnection by was done in 25% of cases, with 65% corresponding to circumferential disconnection and 10% to circumferential disconnection with voltage reduction. In 7 procedures, the superior vena cava was also electrically disconnected.
In 80% of these procedures, an irrigated tip was used, in 15% an 8-mm tip was used, and in 5% cryoablation was used.
A total of 61 complications (5.1%) was reported: significant pericardial effusion/cardiac tamponade (30), acute coronary syndrome (1), vascular access (16), cerebrovascular accident (5), phrenic paralysis (3), upper digestive hemorrhage (1), pulmonary vein stenosis (3), transient gastric paralysis (1), and mitral entrapment of the circular catheter requiring surgery (1). There was 1 death after respiratory distress.
Idiopathic Ventricular Tachycardia
A total of 190 ablation procedures for IVT was reported from 47 centers (mean, 4 [range, 1-17] ablations per site). Success was achieved in 137 procedures (72.1%) and only 4 complications (2%) occurred: 3 tamponades and 1 femoral pseudoaneurysm.
The type of ventricular tachycardia was known in 165 procedures: 101 occurred in the right ventricular outflow tract, 33 in the left ventricular outflow tract, 13 were fascicular, and 18 were reported as occurring in "another location." Success rates were 83%, 76%, 69%, and 83%, respectively.
In most cases (80%), the ablation catheter tip used was 4 mm.
Ventricular Tachycardia With Post-Infarction Scarring
A total of 40 (68%) centers performed 240 VT-AMI ablation procedures (mean, 6; [range, 1-38] ablations per site). The following complications (n=13, 5.4%) were reported: vascular access (7), cardiac tamponade (3), cerebrovascular accident (1), acute heart failure (1), and acute coronary syndrome (1).
The type of ablation was reported in 203 cases: 92 used a "conventional" approach and 111 were substrate specific. In 198 cases, a non-standard catheter tip was used: 51 were 8-mm tip and 147 irrigated tip.
The success rate reported using the conventional approach (noninducibility of clinical tachycardia after ablation) was 79.3%. An epicardial approach was used to treat the ventricular tachycardia in 4 cases.
Ventricular Tachycardia Without Post-Infarction Scarring
Ninety-seven ablation procedures were performed for this condition, in 27 laboratories (46%). Two complications were reported: a vascular complication and cardiac decompensation.
The following types of tachycardia were treated: 17 arrhythmogenic right ventricular dysplasias, 8 branch-branch, 26 nonischemic dilated cardiomyopathies, and 19 reported as "other." Success rates were 70.5%, 100%, 61%, and 84%, respectively. There was one epicardial procedure.
In 39% of the procedures, a nonstandard catheter was used: in 2 cases, an 8-mm catheter tip was used and in 36 cases an irrigated catheter tip was used.
DISCUSSION
As in previous years, 2009 saw a steady increase in activity in arrhythmia units in Spain. The record participation in this year's Registry, both in terms of the number of participating hospitals (59) and the number of procedures performed (the figure of 8500 procedures was exceeded for the first time), ensures that the data obtained were representative. It should be pointed out, however, that the number of ablations this year was 10.4% higher than the previous year, a figure that exceeds the upward trend of previous years. Last year, we "complained" that 10% of centers only sent in the number of procedures performed, without stating the outcomes, the complications reported, catheters used, and characteristics of the substrate. However, this year, that figure has decreased considerably, something worthy of praise.
The increase in the number of ablations this year once again contrasts with the nonexistent increase in human and technical resources, something that is becoming all too familiar year after year. The figures for physicians, nurses, students, etc, are the same as for 2008, despite the increase of more than 10% in the number of ablations. This is coupled with the extra burden taken on by some laboratories that also implant devices.
The distribution of substrates this year shows some particular features that should be discussed. On the one hand, for the so-called conventional substrates, the number of procedures seems to have stabilized, and CTI is once again the second-most frequent substrate treated in absolute terms. Among these conventional substrates, AVN ablation continues to increase (16% this year), probably because it is a useful option in certain patients who fail more complex procedures. In the case of the so-called complex substrates, there are 2 distinct trends. On the one hand, we believe that AF ablation has become established, as reflected by the more than 1000 procedures undertaken, a 44% increase compared to 2008. Moreover, the rate of complications remained stable and this substrate is now one of the main substrates treated in many laboratories in Spain. This increase in the number of AF ablations is accompanied by an increase (of 40%) in ablation procedures for MAT, which usually arises after ablation for atrial fibrillation. We should also highlight that some centers have initiated programs of AF ablation based on cryoenergy and other alternative energy sources. It remains to be seen whether these energy sources become established.9-10
However, we should also draw attention to a noteworthy stability, which is perhaps a disappointment, in the number of ventricular tachycardia ablations. Unlike atrial ablation, ablation of VT-AMI has not become established and fewer such ablations were performed this year than last year. Moreover, the maximum range of ablations of VT-AMI has also decreased notably, from 38 to 14. In the coming years, we shall see whether improved navigation and imaging techniques will suffice to reverse this trend.11 Likewise, the other 2 types of ventricular tachycardia substrate— diopathic and nonischemic—have remained stable.
CONCLUSIONS
The 2009 Spanish Catheter Ablation Registry, as in previous years, includes one of the largest samples published to date in the international literature on ablation procedures, and noticeably exceeds the 7700 ablations performed the year before. The high participation rate, with the collaboration of 59 electrophysiology laboratories, makes the data obtained on the activity and the results of this procedure in Spain extremely reliable. The success rate of ablation procedures in Spain remains high (>90%) with low levels of major complications (<2%) and mortality (0.046%). Ablation of atrial fibrillation has undergone the largest increase in the number of procedures, reflecting a substantial advance compared to previous years. CTI ablation for treatment of typical atrial flutter remained stable as the second most frequently treated substrate, followed by ARTN. In addition, the number of ablation procedures for ventricular tachycardias increased minimally, if at all.
ACKNOWLEDGMENTS
The Registry coordinators would once again like to express their appreciation to all those who participated in the 2009 Ablation Registry, and who voluntarily and selflessly sent data on their procedures. They also thank Cristina Plaza for her excellent and tireless administrative work.

ABBREVIATIONS
AF: atrial fibrillation
ANRT: atrioventricular nodal reentrant tachycardia
AP: accessory pathway
AT: atrial tachycardia
CTI: cavotricuspid isthmus
IVT: idiopathic ventricular tachycardia
VT-AMI: ventricular tachycardia with postinfarction scar
VT-NAMI: ventricular tachycardia associated with nonischemic heart disease
A list of centers and clinicians participating in the 2009 Spanish Catheter Ablation Registry is provided at the end of the article.
Correspondence: Dr. I. García-Bolao.
Irunlarrea, 13, 8.o-D. 31008 Pamplona. Navarra. Spain
E-mail: igarciab@unav.es