

This report presents updated data on heart transplants in Spain, including procedures carried out in 2024. It reviews trends over the past decade (2015-2024) in donor and recipient characteristics, surgical techniques, immunosuppression strategies, and survival rates.
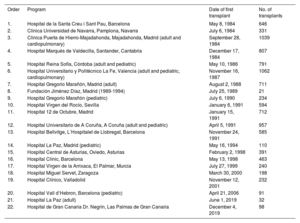
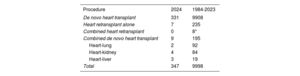
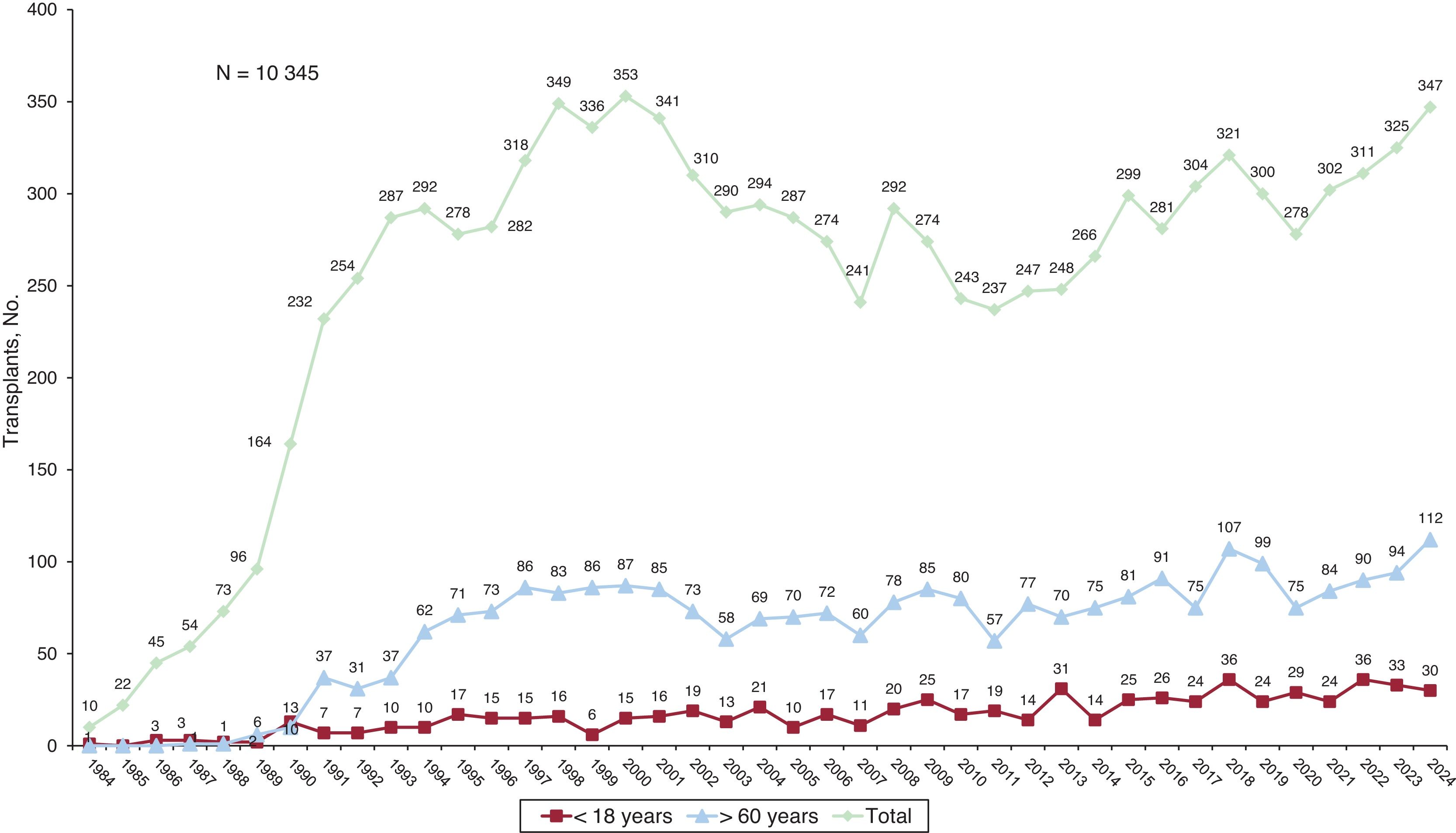
MethodsData were drawn from the Spanish heart transplant registry, which is updated annually. The analysis includes 347 transplants performed in 2024, as well as procedures from 2015 to 2023 (n=2721).
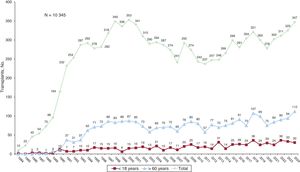
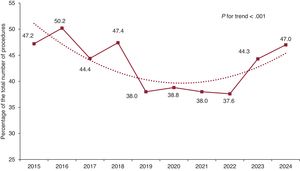
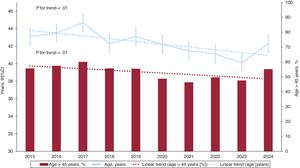
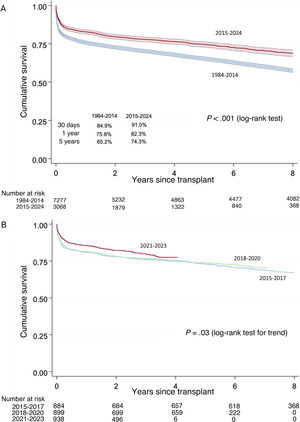
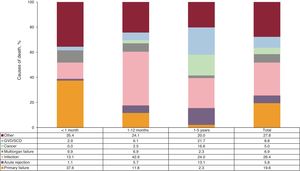
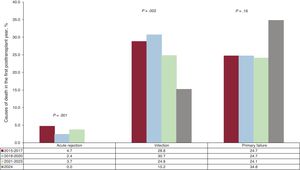
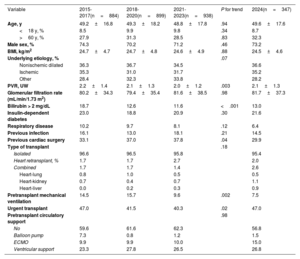
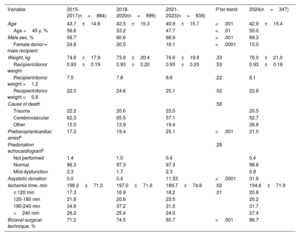
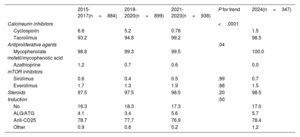
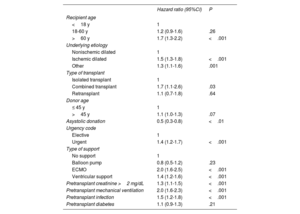
ResultsIn 2024, the number of heart transplants increased by 6.8% compared with 2023. There were no significant changes in recipient age or sex, but the proportion of urgent transplants rose to 47.0%. Use of circulatory support devices increased, particularly extracorporeal membrane oxygenation. The average donor age showed a slight increase in 2024, although the long-term trend remained downward. Donation after circulatory death accounted for 29.1% of transplants in 2024. One-year survival rates improved, reaching 85.2% for transplants performed between 2021 and 2023.
ConclusionsThe number of heart transplants continued to grow, nearing historic highs, largely due to the expansion of donation after circulatory death. Improved 1-year survival reflects the maturity of transplant programs, advances in surgical and medical management, and better pretransplant conditions in recipients.
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm