Keywords
INTRODUCTION
Aortic regurgitation is usually a diastolic phenomenon. However, it has been found during ventricular systole with some arrhythmias1,2 and in situations with unusual circulatory physiology such as assisted circulation1 and after palliation of complex congenital heart diseases.3
There are very few descriptions of systolic aortic regurgitation (Sys-AR) and the frequency and clinical associations of the phenomenon are unknown. After observing Sys-AR in the echocardiograms of several patients in our laboratory, we decided to study its incidence and the clinical characteristics of the patients presenting with this phenomenon.
METHODS
Exhaustive, prospective review of all the studies performed during 1 month in a transthoracic echocardiography unit in patients hospitalised in a general university hospital. Sys-AR was defined as the presence of blood flow (detected by colour or spectral Doppler) from the aorta to the left ventricular outflow tract during a complete systole registered on the electrocardiographic lead of the echocardiograph. In patients with any degree of aortic regurgitation, a 120 s continuous Doppler spectrum study was made of the aortic regurgitation flow using an apical window. The degree of aortic regurgitation was classed as mild, moderate or severe by determining the width of the regurgitation jet in relation to the diameter of the left ventricular outflow tract and/or the measurement of the vena contracta.4 Clinical data was obtained from the patients' medical records.
RESULTS
Within the study period, electrocardiograms were performed on 216 patients (Table 1), among whom we detected 5 (2.3%) cases of Sys-AR. Sys-AR presented in 5.9% of the 84 patients admitted with heart failure as the main or secondary diagnosis. Figure 1 shows images representing the Sys-AR phenomenon. In all cases, aortic regurgitation was class I or II on IV. Table 2 shows the clinical characteristics of the cases. Two striking echocardiographic images from the first patient in the series have been shown elsewhere.5 Case number 5 in the table refers to a male aged 55 with chronic atrial fibrillation (AF), controlled arterial hypertension and prior alcoholism, hospitalised for mild chronic heart failure and treated with acenocoumarol, furosemide, spironolactone, losartan, bisoprolol, and digoxin. The patient had previously been subjected to external electrical cardioversion with early recurrence of arrhythmia in spite of treatment with amiodarone. At the time the patient was admitted, he had not taken antiarrhythmic agents for 1 year aimed at a strategy for the pharmacological control of his ventricular response. The electrocardiogram on admission showed normal ventricles, a left ventricular ejection fraction of 50%, left atrial dilatation, and aortic regurgitation with Sys-AR phenomenon (Figure 2A) in ventricular beats with short R-R. The discovery of Sys-AR in the echocardiogram revealing mechanical inefficiency caused by arrhythmia motivated a Holter study aimed at identifying dual AF nodal physiology using the frequency histogram,6 which was proven in this case. Atrioventricular (AV) node modulation was successfully carried out by slow pathway ablation7 with a cryoablation catheter performed on an outpatient basis after clinical stabilisation. Six weeks after the procedure, an echocardiogram showed the Sys-AR phenomenon had disappeared (Figure 2B). In a Holter on the same day, the frequency histogram showed the slow pathway conduction had ceased. Within this time, and without any changes to the medical treatment or lifestyle, the patient´s overall subjective clinical condition improved. Average heart rate reduced from 88 to 76 beats/min, N-terminal pro-B-type natriuretic peptides (NT-proBNP) reduced from 1011 to 432 pg/mL, and went from doing 8 to 13 minutes of exercise in both cardiac stress tests limited by symptoms with the modified Bruce protocol, carried out 1 week before and 6 weeks after the electrophysiological procedure.


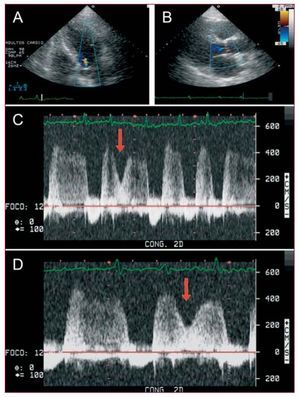
Figure 1. A and B: colour Doppler echocardiographic images in apical 5-chamber and parasternal long axis views respectively, showing the aortic regurgitation flow during the systole. C and D: continuous Doppler spectrum from the left ventricular outflow tract obtained from an apical position of the transducer, in which the second QRS complex is followed by a reduction in the aortic regurgitation flow rate by the mechanical ventricular activity (red arrows), but without anterograde aortic flow. The aortic regurgitation flow persists throughout the entire systole.


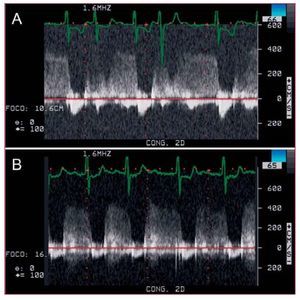
Figure 2. Continuous Doppler spectrum obtained from an apical 5-chamber view of the left ventricular outflow tract in patient 5 in Table 2. A: it can be seen that the second and fourth beats do not generate sufficient pressure to generate anterograde flow, with the consequential persistence of aortic regurgitation flow in the systole. B: spectrum obtained 6 weeks after the atrioventricular node cryomodulation, with suppression of the R-R short intervals and the systolic aortic regurgitation phenomenon.
DISCUSSION
Sys-AR is explained as the inability of the aortic valve to function effectively and the inability of the left ventricular beat to generate sufficient pressure to overcome the aortic pressure.1,2 After a short R-R interval, the systolic pressure generated by the left ventricle fails to reach the aortic pressure required to open the aortic valve. This means that the aortic pressure is higher than the left ventricular pressure throughout the cycle and the aortic regurgitation flow persists during systole. As shown by the arrows in Figure 1, during the ventricular systole, the speed of aortic regurgitation decreases because left ventricular pressure manages to decrease the pressure gradient between the aorta and the left ventricle, but without overcoming aortic pressure, meaning no anterograde flow is produced. Kronzon et al2 offer a pressure diagram that facilitates understanding of the haemodynamics of the phenomenon.
In our study we show that this is not an unusual finding in the conventional transthoracic echocardiography performed on hospitalised patients. The Sys-AR shows the mechanical inefficiency of some beats and may be a simple way of showing mechanical ventricular alternation. Sys-AR is theoretically influenced by reduced ventricular contractility, ventricular filling, left ventricular pressure, and diastolic arterial pressure (DAP). In our patient series, ventricular function was, at most, lightly depressed and we found no serious increases in DAP. In 1 case, mitral stenosis may have contributed to poor ventricular filling and, in another mitral regurgitation may have favoured the loss of left ventricular pressure. But in all cases, the common factor is arrhythmia with short diastole prior to the Sys-AR. A mild degree of aortic regurgitation would theoretically favour Sys-AR as it contributes little to ventricular filling in these cases. In our series, aortic regurgitation was of mild degree in all cases.
One important piece of information is that we observed Sys-AR in patients with a clinical diagnosis of heart failure. The isolated case published providing information about the symptomatic status reported dyspnoea as the reason for the consultation,2 which was in keeping with our findings. The phenomenon therefore seems to show some specificity for heart failure, although it would be necessary to study larger populations to confirm this and assess its diagnostic usefulness.
The echocardiographic finding of Sys-AR with occasional mechanical inefficiency in 1 patient with chronic atrial fibrillation led us to perform a Holter study to assess the ventricular response and the presence of dual nodal physiology.6 Modulation of the AV node (by slow pathway ablation) using a cryoablation catheter managed to eliminate the shorter R-R beats and increased mechanical efficiency was found with the disappearance of Sys-AR (Figure 2), accompanied by clear symptomatic improvement and reduction of NT-proBNP. AV node modulation could be a therapeutic option for these patients.7
The availability and use of cryoablation catheters has recently increased in electrophysiology laboratories,8 partly because they offer greater safety. We show that the use of cryoablation for AV node modulation is, therefore, a feasible alternative. Its effectiveness, the increased safety in comparison to radiofrequency modification of the AV node and the use of the echocardiographic finding of Sys-AR for detecting patients in atrial fibrillation with dual AV node physiology that could benefit from this treatment would require specific studies.
In conclusion, systolic aortic regurgitation is not an exceptional finding in routine hospital clinical practice. It presents with some specificity in patients with clinical heart failure. The use of its detection in the diagnosis, prognosis and the therapeutic guide for heart failure has not yet been determined.
Correspondence: Dr. D.R. Saura Espín.
Puerta de Orihuela, 3 bis; 7.o D. 30003 Murcia. España.
E-mail: danielsaura@secardiologia.es
Received September 1, 2007.
Accepted for publication November 15, 2007.