According to the European guidelines, the cephalic vein cut-down technique and axillary vein (AV) access are recommended as the first-line approach for transvenous cardiac implantable electronic device (CIED) implantation.1 AV catheterization can be performed using surface landmarks, fluoroscopic guidance (FG), with or without venography, or ultrasound imaging.2 Compared with ultrasound guidance, FG may increase the risk of collateral damage (inadvertent arterial puncture or pneumothorax). In a recent single-center retrospective trial comparing ultrasound-guidance with FG-AV access for single or dual chamber CIED first implant, performance was similar, but with higher radiation exposure in the FG group.3 We conducted a multicenter randomized controlled study to compare the performance, safety, and radiation exposure of ultrasound-guided vs FG-AV access for CIED implantation.
From November 2020 to November 2021, we included all consecutive patients eligible for transvenous CIED implantation (by 4 operators) in 3 participating centers (patients were excluded if younger than 18 years, or required battery revision only). We analyzed single, dual chamber, cardiac resynchronization therapy pacemakers and defibrillators, and upgrade procedures. Of 4 operators, 3 were electrophysiologists practicing CIED implantation for more than 10 years (> 200 cases with ultrasound for the first;>200 cases with FG for the second;>100 cases with ultrasound for the third), and 1 was a less experienced electrophysiology fellow (> 50 procedures with ultrasound, and<20 cases with FG). A time limit for AV catheterization attempts was set to 15minutes after which a crossover could be performed for the other arm. If both the ultrasound and FG techniques failed, the cephalic vein technique was used as a second option, and subclavian vein access as the last option. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the human research committee of participating institutions. All patients provided written consent for enrollment in the registry and the study.
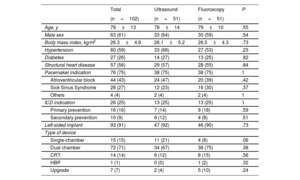
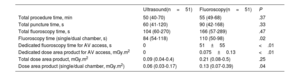
After the roll-in period (5 patients), 102 patients (n=51 patients per group) were included (table 1). A total of 99 leads were implanted in the ultrasound group and 96 in the FG group. AV catheterization was successfully performed in 50/51 patients (98%) in the ultrasound group and in 49/51 patients in the FG group (96%; P=.56). The mean number of access attempts was 1.17 per lead in the ultrasound group vs 1.14 per implanted lead in the FG group (P=.96). Of note, the overall percentage of patients requiring the 2 x 1 technique (single access for 2 leads) was 20% in the ultrasound group vs 17% in the FG group (P=.54). In the ultrasound group, AV access time and procedure time were shorter than in the FG group, but without reaching significance, respectively: 60seconds (interquartile range [IQR], 41-120) vs 90seconds (IQR, 42-168); P=.33; 50minutes (IQR, 40-70) vs 55min (IQR, 49-68min); P=.37. Total fluoroscopy time and total dose area product (DAP) were lower in the ultrasound group, but without reaching significance (table 2). In the subgroup of patients with single or dual chamber CIED, this difference became statistically significant in favor of the ultrasound group. DAP was also lower in the ultrasound group than the FG group. There were 2 major complications in each group during the 16±6 months of follow-up: 1 pocket hematoma and 1 pocket infection in each group. All patients were alive at the 12-month follow-up visit.
Patient characteristics
| Total | Ultrasound | Fluoroscopy | P | |
|---|---|---|---|---|
| (n=102) | (n=51) | (n=51) | ||
| Age, y | 79±13 | 78±14 | 79±10 | .55 |
| Male sex | 63 (61) | 33 (64) | 30 (59) | .54 |
| Body mass index, kg/m2 | 26.3±4.8 | 26.1±5.2 | 26.5±4.3 | .73 |
| Hypertension | 60 (59) | 33 (68) | 27 (53) | .23 |
| Diabetes | 27 (26) | 14 (27) | 13 (25) | .82 |
| Structural heart disease | 57 (56) | 29 (57) | 28 (55) | .84 |
| Pacemaker indication | 76 (75) | 38 (75) | 38 (75) | 1 |
| Atrioventricular block | 44 (43) | 24 (47) | 20 (39) | .42 |
| Sick Sinus Syndrome | 28 (27) | 12 (23) | 16 (30) | .37 |
| Others | 4 (4) | 2 (4) | 2 (4) | 1 |
| ICD indication | 26 (25) | 13 (25) | 13 (25) | 1 |
| Primary prevention | 16 (16) | 7 (14) | 9 (18) | .59 |
| Secondary prevention | 10 (9) | 6 (12) | 4 (8) | .51 |
| Left-sided implant | 93 (91) | 47 (92) | 46 (90) | .73 |
| Type of device | ||||
| Single-chamber | 15 (15) | 11 (21) | 4 (8) | .06 |
| Dual chamber | 72 (71) | 34 (67) | 38 (75) | .38 |
| CRT | 14 (14) | 6 (12) | 8 (15) | .56 |
| HBP | 1 (1) | 0 (0) | 1 (2) | .32 |
| Upgrade | 7 (7) | 2 (4) | 5 (10) | .24 |
CRT, cardiac resynchronization therapy; HBP, His-bundle pacing; ICD, implantable cardioverter defibrillator.
Values are expressed as No. (%) or mean±standard deviation.
Radiation exposure data and implantation procedure time
| Ultrasound(n=51) | Fluoroscopy(n=51) | P | |
|---|---|---|---|
| Total procedure time, min | 50 (40-70) | 55 (49-68) | .37 |
| Total puncture time, s | 60 (41-120) | 90 (42-168) | .33 |
| Total fluoroscopy time, s | 104 (60-270) | 166 (57-289) | .47 |
| Fluoroscopy time (single/dual chamber, s) | 84 (54-118) | 110 (50-98) | .02 |
| Dedicated fluoroscopy time for AV access, s | 0 | 51±55 | <.01 |
| Dedicated dose area product for AV access, mGy.m2 | 0 | 0.075±0.13 | <.01 |
| Total dose area product, mGy.m2 | 0.09 (0.04-0.4) | 0.21 (0.08-0.5) | .25 |
| Dose area product (single/dual chamber, mGy.m2) | 0.06 (0.03-0.17) | 0.13 (0.07-0.39) | .04 |
AV, axillary vein.
The data are expressed as mean±standard deviation, or median [Q1-Q3].
This is the first randomized clinical trial comparing AV puncture techniques using either ultrasound or FG for CIED implantation. In agreement with results reported by Tagliari et al.4 (97%), our study confirms the high success rate of the ultrasound technique (98%). The radiation dose using ultrasound-guided catheterization was decreased by 57% in our global population, although this result was not statistically significant. When considering single or dual chamber CIED implantations with ultrasound-guided AV access, DAP was divided by 2 in our study compared with the FG group (P=.04). Our results on fluoroscopy time confirm those published by Migliore et al., with a significant decrease using ultrasound vs FG.3
Our study demonstrates that, in a population referred for CIED first implant or upgrade procedure, ultrasound guidance and FG have similar performance, with a high success rate (> 95%) and a similar complication rate (2%). Compared with FG, ultrasound guidance reduces the radiation exposure required for AV access to 0, and decreases total radiation exposure, although this result was not significant.
FUNDINGNo funding.
AUTHORS’ CONTRIBUTIONSConceptualization, methodology, validation, formal analysis, writing-review and editing: S.S. Bun. Investigation: P. Taghji, F. Squara and P. L. Massoure. Writing-original draft preparation: P. T Taghji, S.S. Bun. Visualization: F. Squara and P. Taghji. Supervision: J.C. Deharo and E. Ferrari.
CONFLICTS OF INTERESTThe authors have nothing to disclose.