Cardiac imaging is one of the basic pillars of modern cardiology. The potential list of scenarios where cardiac imaging techniques can provide relevant information is simply endless so it is impossible to include all relevant new features of cardiac imaging published in the literature in 2012 in the limited format of a single article. We summarize the year's most relevant news on cardiac imaging, highlighting the ongoing development of myocardial deformation and 3-dimensional echocardiography techniques and the increasing use of magnetic resonance imaging and computed tomography in daily clinical practice.
Keywords
.
ECHOCARDIOGRAPHYUpdate on EchocardiographyThe most important publication of the year deals with the criteria for appropriate use1 and represents a major drive to use this technique rationally.
Technically, the major innovation is the progressive introduction of pocket-size hand-held devices. A consensus document has been published that specifies the indications and type of training recommended for their use,2 while different studies have shown their usefulness in clinical practice3 and in teaching.4 In the foreseeable future, the number of these devices will increase rapidly and they will even be linked with smartphone applications.5
This year has seen a discreet revival in the use of backscatter signal, which can characterize tissues from the echocardiographic image. For example, in patients with hypertrophic cardiomyopathy, cyclical variation of the backscatter signal can be useful in predicting events,6 whereas in dilated cardiomyopathy it can predict inverse remodeling and the degree of fibrosis.7
No major innovation has appeared in other fields. A tool to determine the properties of myocardial contractility has been developed, based on so-called shear wave imaging,8 and analytical systems are being created to study left ventricular rotation dynamics.9 A system enabling us to follow contrast bubbles in order to analyze intracavity flow has also been developed.10
Stress EchocardiographyIn dobutamine stress echocardiography, the troponin concentration is not elevated so its use provides no additional information to help interpret the studies; therefore, it is not recommended.11 Stress echocardiography itself has shown that studying images of peak treadmill exercise is the most sensitive approach as it enables us to see ischemia most frequently and most extensively.12 It has also been shown that a significant proportion of patients with exertional dyspnea and normal ejection fraction (EF) have relevant diastolic dysfunction only during exercise,13 hence they would be not be identified by the criteria in current clinical practice guidelines.
Contrast MediaTransesophageal echocardiography (TEE) continues to be superior to cardiac computed tomography (cardiac CT) in the diagnosis of patent foramen ovale.14 However, TEE is less sensitive than transthoracic echocardiography (TTE) and transcranial Doppler and tends to underestimate shunt.15 Use of contrast enables us to determine the presence of microvascular damage in acute coronary syndrome and this damage has been shown to be reversible, which associates it with a favorable prognosis.16 Contrast media have been combined with exertion in new techniques like 3-dimensional (3D) echocardiography and with new drugs like regadenoson in myocardial perfusion studies.17 Finally, new data have appeared which confirm that contrast perfusion studies add important prognostic information to pharmacologic stress tests.18
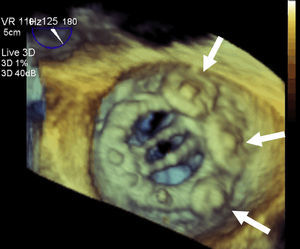
Interventional CardiologyInterventional cardiology in structural heart disease has grown considerably, with increasing use of imaging techniques in selecting suitable patients and procedure monitoring. The European Association of Cardiovascular Imaging (before European Association of Echocardiography) and the American Society of Echocardiography have prepared a joint document of recommendations for the use of echocardiography in these procedures19 which particularly highlights the value of 3D TEE (Fig. 1). Together with transcatheter aortic valve implantation, the other innovation is percutaneous atrial appendage occlusion, in which the opportunity to use 3D TEE improves results.20
VALVULAR HEART DISEASEAortic Valve deployed to treat a perivalvular leak.")
The debate about low-flow low-gradient aortic stenosis with normal EF continues. In a new prospective study, patients with this pattern presented more severe stenosis and data indicating incipient ventricular infection with reduced longitudinal strain, which would explain their poor prognosis.21
One relatively new topic is the evaluation of pulmonary hypertension associated with aortic stenosis, which is found in ≤30% of patients.22 The appearance of pulmonary hypertension with exercise in patients with severe asymptomatic aortic stenosis has prognostic value, hence it could be useful when making decisions on surgery.23 Pulmonary hypertension is associated with greater mortality in patients undergoing valve replacement,24 although the degree of pulmonary pressure does not condition mortality and in the presence of elevated capillary pressure can decline after valve replacement.25
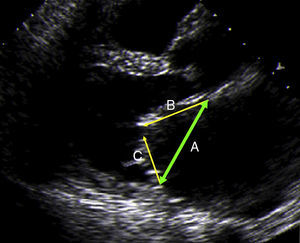
Mitral ValveIn the field of rheumatic mitral stenosis, an interesting index has been described. The >50% ratio between posterior and anterior leaflet length is an excellent predictor of good results in valvuloplasty26 (Fig. 2).

Mitral regurgitation has been associated with diminished exercise capacity in patients with heart failure and ventricular dysfunction.27 In the clinically difficult context of treating mitral regurgitation in patients who undergo aortic valve replacement, prosthesis size mismatch has been shown to limit the expected improvement in the mitral valve lesion, which obliges us to optimize the surgical strategy.28 On the other hand, in patients undergoing aortic valve replacement, moderate mitral regurgitation in the postoperative period is associated with greater mortality during follow-up.29
Studies continue to appear that confirm the advantage of 3D imaging in analyzing valves requiring complex surgery30,31 and in the presurgical study of functional mitral regurgitation32 as they identify the valvular condition precisely33 and enable us to determine the best position of the papillary muscles and assess the need for relocation associated with annuloplasty, which improves surgical results.34
Tricuspid ValveTwo new studies of patients undergoing degenerative mitral regurgitation repair35 or replacement for rheumatic mitral stenosis36 have shown that, although the mild-to-moderate tricuspid regurgitation repair entailed is not accompanied by clear differences in the rates of mortality or need for new surgery, patients without tricuspid valve repair presented greater incidence of moderate-to-severe tricuspid regurgitation in the follow-up and worse event-free survival, which means that adding tricuspid valve repair to mitral valve surgery is recommendable.
Prosthetic ValvesTwo new, relatively simple parameters have been identified (acceleration time>100ms and acceleration time/ejection time ratio>0.37ms) that help detect prosthetic aortic valve stenosis.37
LESIONS OF THE AORTAYoung patients with stroke attributable to patent foramen ovale present larger aortic root diameters than healthy control subjects, which indicates a possible relationship to aortic dilatation.38 In patients with severe aortic stenosis, a relationship exists between the complex atherosclerotic plaque in the aortic arch and cerebral infarction after hemodynamic study or valve replacement.39
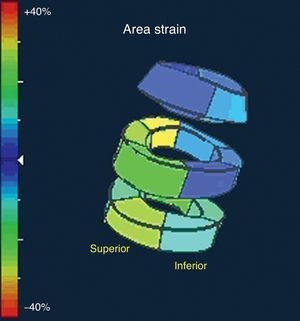
VENTRICULAR FUNCTIONStudy of the ventricular mechanism using deformation parameters continues to develop apace despite its slow implantation in daily clinical practice. The publication of an excellent review article on its usefulness in coronary disease, which clearly summarizes its possible applications, stands out.40 On the other hand, the problem of reproducibility and the standardization of these parameters is being toned down by the recent publication of the normal reference values.41 New tools based on 3D strain have shown its usefulness in studying ventricular function and volume,42–44 although their comparative reproducibility by teams from different commercial companies is again its principle limitation.45 Promising new parameters have appeared, for example area strain (Fig. 3), which combines the longitudinal and circumferential deformations. Initial reports evaluate its usefulness in studying ventricular function.46
CARDIOMYOPATHY
The need to combine information from different imaging techniques has been made clear and deformation parameters have been shown to be useful in several conditions. In patients with hypertrophic cardiomyopathy, simple parameters such as global strain have been proven to be independent predictors of the presence of fibrosis and the risk of adverse events.47 Deformation parameters could also be useful in cardiomyopathy secondary to chemotherapy, in which early decrease in longitudinal strain has been related with cardiotoxicity at 6-month follow-up.48,49
HEART FAILURE AND RESYNCHRONIZATIONThe role of echocardiography in diagnosing heart failure is reflected in the new European Society of Cardiology guidelines,50 which highlight the method of calculating EF and emphasize the usefulness of contrast media, 3D echocardiography and deformation techniques in the evaluation of ventricular function.
Speckle tracking is a promising technique in the identification of ventricular asynchrony. The MUSIC multicenter study concludes that the echocardiography enables us to identify resynchronization responders among patients with and without ischemia.51 Another novel issue is the suggestion that the effectiveness of resynchronization could be related to viability defined by using deformation techniques to study the segment where the electrode is placed.52,53 Three-dimensional echocardiography is another tool that enables us to determine the presence of asynchrony with tissular synchronization techniques, real-time 3D imaging and the 3D study of myocardial deformation and obtain a reliable prediction of response to resynchronization therapy.54,55
NUCLEAR CARDIOLOGYThe technical advances aimed at reducing acquisition time and radiation dose and improving image quality56,57 with cardiac-dedicated single-photon emission computed tomography (SPECT) cameras are being held back in Spain as a consequence of the current economic crisis. Partly for the same reason, positron emission tomography (PET) has not become established in Spain despite the proliferation of PET-CT cameras in oncology.
A substantial number of more recent articles have focused on studying gated myocardial perfusion SPECT in subgroups of asymptomatic patients: with diabetes,58 advanced kidney failure,59 a family history of early heart disease,60 aged>80 years61 and as a preoperative evaluation.62 The use of SPECT with this patient type is not in the guidelines and constitutes one of the most frequent inappropriate uses of the technique.63 This is of special interest if we consider that the impact of noninvasive exploration in therapeutic strategy is only relative.64
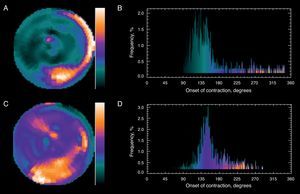
The use of 123I-metaiodobenzyl guanidine scintigraphy to study sympathetic innervation continues to be considered in the risk stratification of patients with heart failure.65,66 Severe arrhythmic events or sudden death are unusual in patients with a heart/mediastinum ratio of>1.6, which could mean that in one fifth of patients with primary indication for an implantable cardioverter-defibrillator67 the implantation might be unnecessary. Another novel idea is the application of Fourier phase analysis to gated myocardial perfusion SPECT (Fig. 4). This is an automatic method that does not depend on the explorer and facilitates the rapid determination of left ventricular asynchrony.68,69
, the phase histogram amplitude increases abnormally. The polar map (B) shows that the greatest delay occurs in the inferior-lateral region of the left ventricle. After cardiac resynchronization therapy (C), the histogram amplitude (D) improves significantly. The patient improved clinically and left ventricular ejection fraction improved from 18% to 32% lower. (Images courtesy of Dr. Santiago Aguadé-Bruix, Hospital Universitari Vall d’Hebron, Barcelona.)")
Fourier analysis of a gated myocardial perfusion single-photon emission computed tomography. Before resynchronization (A), the phase histogram amplitude increases abnormally. The polar map (B) shows that the greatest delay occurs in the inferior-lateral region of the left ventricle. After cardiac resynchronization therapy (C), the histogram amplitude (D) improves significantly. The patient improved clinically and left ventricular ejection fraction improved from 18% to 32% lower. (Images courtesy of Dr. Santiago Aguadé-Bruix, Hospital Universitari Vall d’Hebron, Barcelona.)
The role of hybrid fusion of anatomic and functional images taken with 3D SPECT-CT or PET-CT continues under study because, although they represent a substantial qualitative advance, in practice obtaining these images entails a long processing time. Pazhenkottil et al.70 have indicated that incidence of revascularization in ≤ 60 days following these studies is 41% when hybrid SPECT-CT images show that SPECT and CT findings coincide, 11% when the patterns do not coincide, and 0% if both are normal.
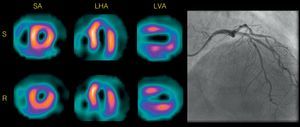
Myocardial viability, which has for years been a source of numerous publications using SPECT and PET, is gradually losing interest although articles on the impact of gated myocardial perfusion SPECT in the indication for catheterization71 and assessment of contractile response to low dosage dobutamine in patients with ischemic cardiomyopathy72 have been published. Pizzi et al.73 have found that the so-called paradoxical scintigraphic pattern (greater uptake during stress than at rest) in regions with myocardial necrosis occurs in territories with scintigraphic criteria of myocardial viability with the responsible artery open (Fig. 5) or with good collateral circulation if the artery is occluded. Although PET is the most effective technique for noninvasive functional diagnosis of coronary disease when taking >50% stenosis in the invasive coronary angiography as a reference, SPECT remains the most widely indicated and validated technique.74
")
Single-photon emission computed tomography myocardial perfusion with 99mTc-tetrofosmin of a patient with chronic anterior infarction and paradoxical scintigraphic pattern, criteria of viability, and permeable anterior descending artery. LHA, long horizontal axis; LVA, long vertical axis; R, rest; S, stress; SA, short axis. (Images courtesy of Dr. M. Nazarena Pizzi, Hospital Universitari Vall d’Hebron, Barcelona.)
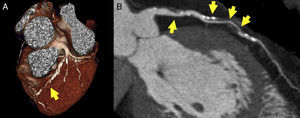
Cardiac CT is now firmly established in clinical practice. With the publication of the CONFIRM study,75 a register with data on >25000 patients showing a clear relationship between the presence and severity of coronary disease diagnosed with cardiac CT and mid-term mortality, the debate over its prognostic value has ended (Fig. 6).
 both in volumetric (A) and multiplanar reconstruction (B). The result has obvious prognostic and diagnostic implications.")
Developments in cardiac CT advance at a tremendous pace. As a technique, it has been shown to be as precise as cardiac magnetic resonance imaging in the assessment of ventricular function.76 An interesting mathematical model has been developed that is capable of noninvasively deriving coronary fractional flow reserve and promises to improve CT performance in coronary disease.77 Moreover, the application of late iodine enhancement is useful in the etiologic diagnosis of dilated cardiomyopathy.78
In clinical practice, two very interesting articles have been published in the New England Journal of Medicine about the usefulness of cardiac CT in assessing the patient with chest pain attending the emergency department. Computed tomography has been shown to be a safe technique that facilitates the diagnosis of a larger number of patients who really have coronary disease and leads to a shorter stay in Emergency and a higher number of direct discharges.79,80 Also this year, the first study appeared with evidence that treatment of asymptomatic patients with baseline risk identified by cardiac CT can reduce the appearance of coronary events. This pioneering study may open the door to changes in the management of coronary disease.81
Finally, cardiac CT is fast gaining acceptance in the assessment of patients suitable for transcatheter aortic prosthesis implantation as data are being gathered that indicate it could prove the most precise way to measure the aortic annulus (and, therefore, select prosthesis size) and that its use could reduce the percentage of patients with postprocedural periprosthetic failure.82,83
CARDIAC MAGNETIC RESONANCE IMAGINGCardiac magnetic resonance imaging has become invaluable in ischemic cardiomyopathy, to the point where the loss of viability of a segment of myocardium has been included in the latest universal definition of myocardial infarction.84 Late gadolinium enhancement is efficient in the etiologic study of dilated cardiomyopathy85 and in prognostic assessment, as myocardial scarring is an efficient risk marker for ventricular arrhythmias.86 The new 3D perfusion sequences have been validated. They perform well and enable us to calculate ischemic burden in the myocardium.87 Strain encoded sequencing is another new technique that promises to improve the sensitivity of dobutamine tests.88
The role of cardiac magnetic resonance imaging in studying the myocardium appears never-ending. In hypertrophic cardiomyopathy, it has been shown that fibrosis is a progressive process associated with the functional stage89 and that intramyocardial fibrosis is a clear predictor of mortality in patients with aortic stenosis.90 Also, left ventricular lesions in right ventricular arrhythmogenic dysplasia have been defined in detail.91 The capacity of cardiac magnetic resonance imaging to describe early abnormalities, such as right ventricular hypertrophy in an apparently healthy population, has been demonstrated.92 Finally, one of the most novel observations of the year has been the demonstration that late enhancement can also be useful in pericardial pathology as it can predict how constrictive pericarditis will respond to antiinflammatory drug treatment.93
CONFLICTS OF INTERESTNone declared.